

Reciprocal changes in cervical spine alignment after corrective thoracolumbar deformity surgery
- PMID: 24136416
- PMCID: PMC3940792
- DOI: 10.1007/s00586-013-2953-8
Reciprocal changes in cervical spine alignment after corrective thoracolumbar deformity surgery
Abstract
Purpose: To identify changes in cervical alignment parameters following surgical correction of thoracolumbar deformity and then assess the preoperative parameters which induce changes in cervical alignment following corrective thoracolumbar deformity surgery.
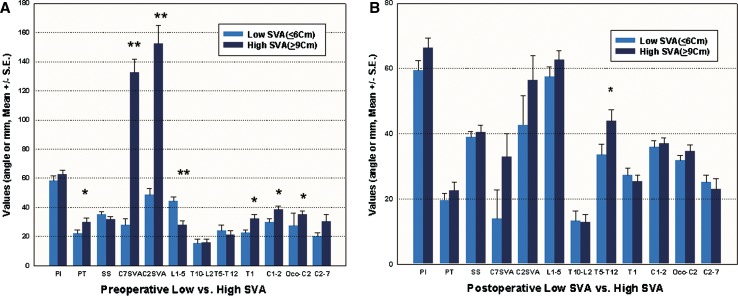
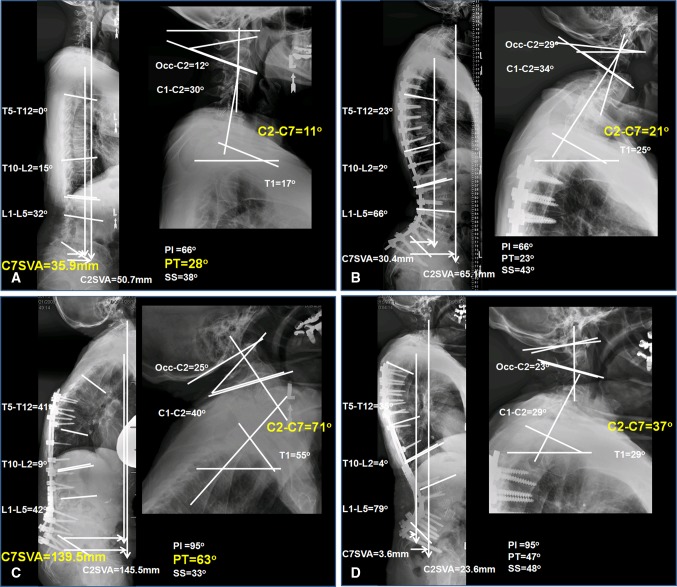
Methods: A retrospective study of 49 patients treated for thoracolumbar deformity with preoperative planning of an acceptably aligned coronal and sagittal plane in each case. We compared cervical spine parameters in two distinct low [preoperative C7 sagittal vertical axis (SVA) ≤ 6 cm] and high (preoperative C7 SVA ≥ 9 cm) C7 SVA groups. Multilinear regression analysis was performed and revealed the relationship between postoperative cervical lordosis and preoperative spinopelvic parameters and surgical plans.
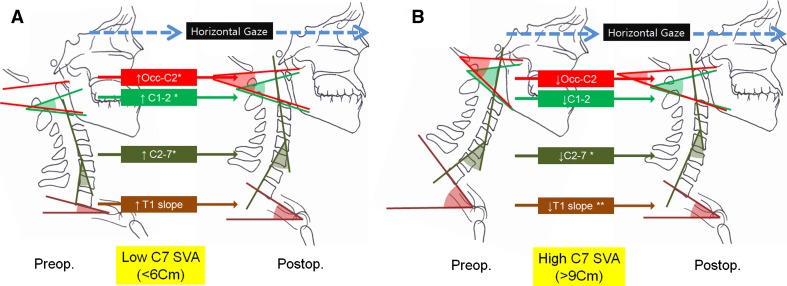
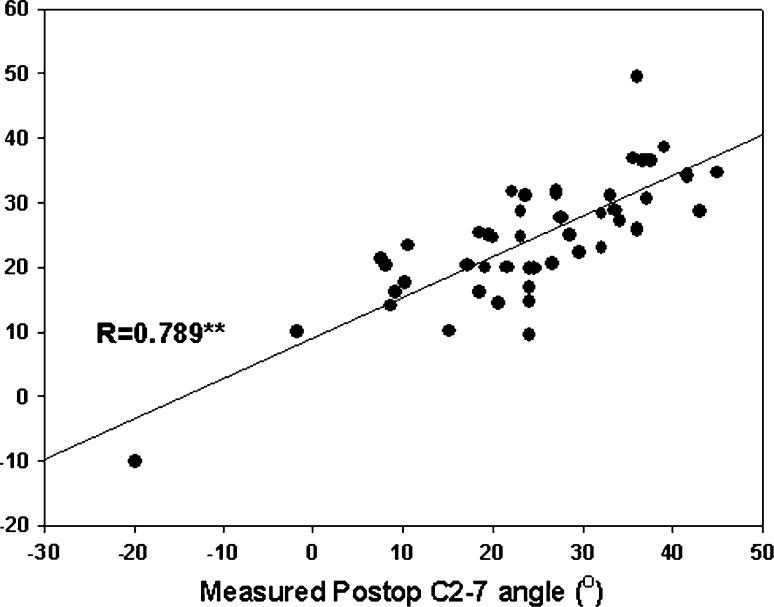
Results: In the lower C7 SVA group, cervical lordosis was significantly increased after thoracic/lumbar deformity correction (p < 0.01). In contrast, the high C7 SVA group showed decreased cervical lordosis postoperatively (p < 0.01). Multilinear regression analysis demonstrated the preoperative parameters (preoperative C2-7 angle, T1 slope, surgical plan for PT and C7 SVA), which determine the postoperative cervical lordosis.
Conclusion: In spinal deformity procedures, preoperative spinal alignment parameters, and surgical plans could affect postoperative cervical spine alignment.
Figures
References
-
- Boulay C, Tardieu C, Hecquet J, Benaim C, Mouilleseaux B, Marty C, Prat-Pradal D, Legaye J, Duval-Beaupere G, Pelissier J. Sagittal alignment of spine and pelvis regulated by pelvic incidence: standard values and prediction of lordosis. Eur Spine J. 2006;15:415–422. doi: 10.1007/s00586-005-0984-5. - DOI - PMC - PubMed
-
- Lafage V, Schwab F, Vira S, Hart R, Burton D, Smith JS, Boachie-Adjei O, Shelokov A, Hostin R, Shaffrey CI, Gupta M, Akbarnia BA, Bess S, Farcy JP. Does vertebral level of pedicle subtraction osteotomy correlate with degree of spinopelvic parameter correction? J Neurosurg Spine. 2011;14:184–191. doi: 10.3171/2010.9.SPINE10129. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
