

Non-invasive versus invasive respiratory support in preterm infants at birth: systematic review and meta-analysis
- PMID: 24136633
- PMCID: PMC3805496
- DOI: 10.1136/bmj.f5980
Non-invasive versus invasive respiratory support in preterm infants at birth: systematic review and meta-analysis
Erratum in
- BMJ. 2014;348:g58
Abstract
Objective: To assess the role of nasal continuous positive airway pressure (CPAP) initiated at birth for prevention of death and bronchopulmonary dysplasia in very preterm infants.
Design: Systematic review.
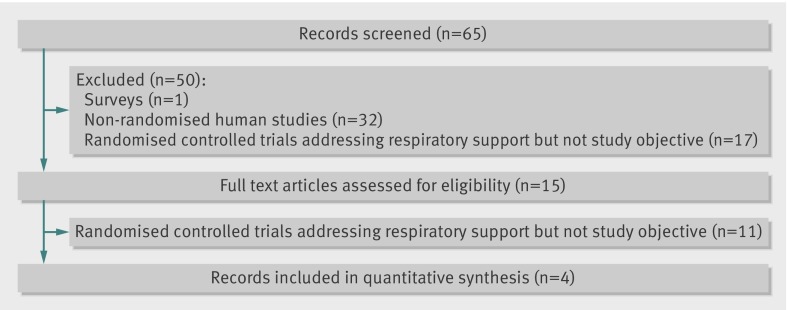
Data sources: PubMed, Embase, the Cochrane Central Register of Controlled Trials, and online Pediatric Academic Society abstracts from the year of inception to June 2013.
Eligibility criteria for selecting studies: Randomised controlled trials evaluating the effect of nasal CPAP compared with intubation in preterm infants born at less than 32 weeks' gestation and presenting the outcomes of either death or bronchopulmonary dysplasia, or both (defined as the need for oxygen support or mechanical ventilation at 36 weeks corrected gestation), during hospital stay.
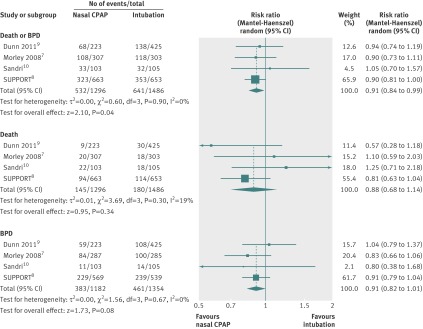
Results: Four randomised controlled trials (2782 participants) met the inclusion criteria, with 1296 infants in the nasal CPAP group and 1486 in the intubation group. All the trials reported bronchopulmonary dysplasia independently at 36 weeks corrected gestation, with borderline significance in favour of the nasal CPAP group (relative risk 0.84, 95% confidence interval 0.68 to 1.04, risk difference -0.02, 95% confidence interval -0.04 to 0.01). [corrected] No difference in death was observed (relative risk 0.88, 0.68 to 1.14, risk difference -0.02, -0.04 to 0.01, respectively). Pooled analysis showed a significant benefit for the combined outcome of death or bronchopulmonary dysplasia, or both, at 36 weeks corrected gestation for babies treated with nasal CPAP (relative risk 0.90 (95% confidence interval 0.83 to 0.98, risk difference -0.04 (95% confidence interval -0.08 to -0.00), NNT [corrected] of 25).
Conclusion: One additional infant could survive to 36 weeks without bronchopulmonary dysplasia for every 25 babies treated with nasal CPAP in the delivery room rather than being intubated.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med 2001;163:1723-9. - PubMed
-
- Baraldi E, Filippone M. Chronic lung disease after premature birth. N Engl J Med 2007;357:1946-55. - PubMed
-
- Kinsella JP, Greenough A, Abman SH. Bronchopulmonary dysplasia. Lancet 2006;367:1421-31. - PubMed
-
- Doyle LW, Faber B, Callanan C, Freezer N, Ford GW, Davis NM. Bronchopulmonary dysplasia in very low birth weight subjects and lung function in late adolescence. Pediatrics 2006;118:108-13. - PubMed
-
- Doyle LW, Anderson PJ. Long-term outcomes of bronchopulmonary dysplasia. Semin Fetal Neonatal Med 2009;14:391-5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous