

Effect of implementing an acute myocardial infarction guideline on quality indicators
- PMID: 24136764
- PMCID: PMC4878596
- DOI: 10.1590/s1679-45082013000300016
Effect of implementing an acute myocardial infarction guideline on quality indicators
Abstract
Objective: To evaluate the compliance rates to quality of care indicators along the implementation of an acute myocardial infarction clinical practice guideline.
Methods: A clinical guideline for acute myocardial infarction was introduced on March 1st, 2005. Patients admitted for acute myocardial infarction from March 1st, 2005 to December 31st, 2012 (n=1,431) were compared to patients admitted for acute myocardial infarction before the implementation of the protocol (n=306). Compliance rates to quality of care indicators (ASA prescription on hospital admission and discharge, betablockers on discharge and door-to-balloon time) as well as the length of hospital stay and in-hospital mortality were compared before and after the implementation of the clinical guideline.
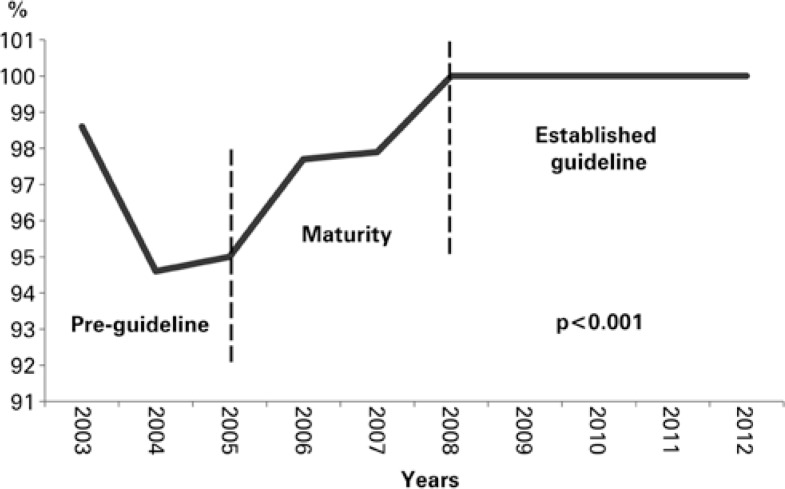
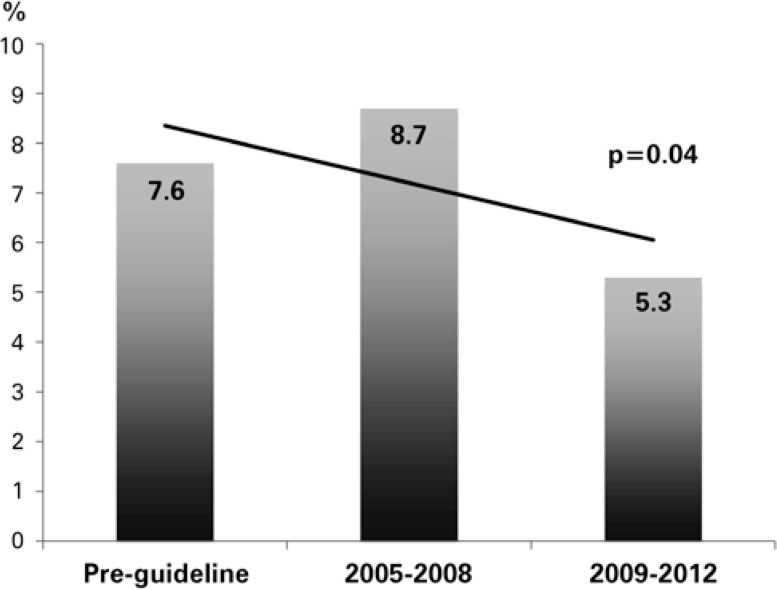
Results: The rates of ASA prescription on admission, on discharge and of betablockers were higher after guideline implementation: 99.6% versus 95.8% (p<0.001); 99.1% versus 95.8% (p<0.001); and 95.9% versus 81.7% (p<0.001), respectively. ASA prescription rate increased over time, reaching 100% from 2009 to 2012. Door-to-balloon time after versus before implementation was of 86(32) minutes versus 93(51) (p=0.20). The length of hospital stay after the implementation versus before was of 6(6) days versus 6(4) days (p=0.34). In-hospital mortality was 7.6% (before the implementation), 8.7% between 2005 and 2008, and 5.3% between 2009 and 2012, (p=0.04).
Conclusion: The implementation of an acute myocardial infarction clinical practice guideline was associated with an increase in compliance to quality of care indicators.
Objetivo:: Avaliar a adesão aos indicadores de qualidade assistencial ao longo da implementação de um protocolo assistencial de infarto agudo do miocárdio.
Métodos:: Em 1º de março de 2005 foi implementado o protocolo assistencial de infarto agudo do miocárdio. Foram selecionados pacientes admitidos de 1º de março de 2005 a 31 de dezembro de 2012 (n=1.431). Para comparação, utilizamos os dados de pacientes admitidos por infarto na fase pré-protocolo (n=306). Comparamos a taxa de adesão aos indicadores (taxa de prescrição de AAS na admissão hospitalar e na alta hospitalar, betabloqueador na alta e tempo porta-balão) entre as fases pré e pós-implementação do protocolo, além de tempo de permanência hospitalar e mortalidade intra-hospitalar nas diferentes fases.
Resultados:: As taxas de prescrição de AAS na admissão e na alta hospitalar, e de betabloqueador foram maiores na fase pós versus a pré-implementação do protocolo: 99,6% versus 95,8% (p<0,001); 99,1% versus 95,8% (p<0,001) e 95,9% versus 81,7% (p<0,001), respectivamente. A taxa de prescrição de AAS aumentou ao longo da implementação do protocolo, atingindo 100% de 2009 a 2012. O tempo porta-balão pós versus pré foi de 86(32) minutos versus 93(51), respectivamente (p=0,20). O tempo de permanência hospitalar foi semelhante na fase pré versus pós-protocolo: 6(6) dias versus 6(4) dias (p=0,34). A mortalidade intra-hospitalar foi de 7,6% no pré-protocolo, 8,7% entre 2005 e 2008 e 5,3% entre 2009 e 2012 (p=0,04).
Conclusão:: A implementação do protocolo assistencial refletiu-se na maior adesão aos indicadores de qualidade.
Conflict of interest statement
Conflicts of interest: none.
Figures
References
-
- Varkey P, Reller MK, Resar RK. Basics of quality improvement in health care. Mayo Clin Proc. 2007;82(6):735–739. - PubMed
-
- Kohn LT, Corrigan JM, Donaldson MS, editors. To err is human. Building a safer health system. Washington, DC: National Academy Press; 2000. - PubMed
-
- US Department of Health and Human Services Agency for Healthcare Research and Quality. Your guide to choosing quality healthcare: a quick look at quality [Internet] [[cited 2013 Aug 26]]. Available from: http://archive.ahrq.gov/consumer/qnt/qntqlook.htm.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
