

Fixation versus replacement of radial head in terrible triad: is there a difference in elbow stability and prognosis?
- PMID: 24136807
- PMCID: PMC4048405
- DOI: 10.1007/s11999-013-3331-x
Fixation versus replacement of radial head in terrible triad: is there a difference in elbow stability and prognosis?
Abstract
Background: Surgical treatment for terrible triad injuries of the elbow (defined as elbow dislocations with concomitant fractures of the radial head and coronoid) remains a challenging clinical problem. Specifically, the question of whether to repair or replace the radial head remains controversial.
Questions/purposes: We compared patients with terrible triad injuries of the elbow whose radial head fracture was treated with either internal fixation and internal fixation (ORIF) or radial head arthroplasty in terms of (1) clinical outcome measures (DASH and Broberg-Morrey scores, ROM), (2) elbow stability and radiographic signs of arthrosis, and (3) complications and reoperation rates.
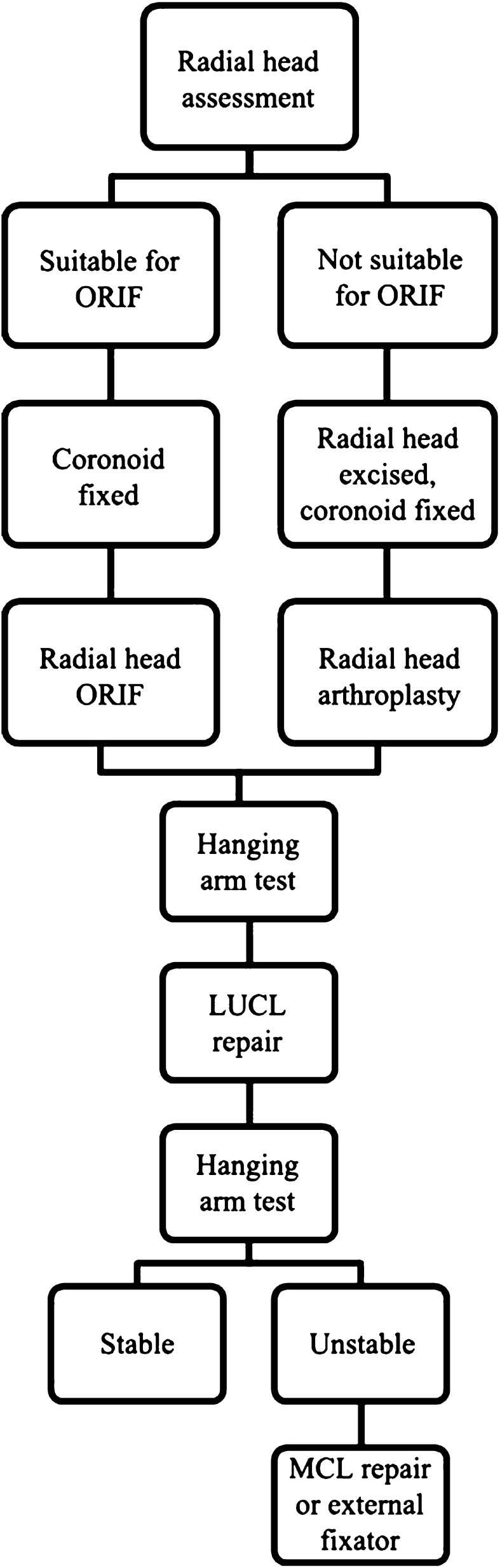
Methods: Retrospective review identified 39 patients with terrible triad injuries and minimum 18-month complete clinical and radiographic followup (mean, 24 months; range, 18-53 months). Patients were managed with a standard algorithm consisting of (1) repair (n = 9) or replacement (n = 30) of the radial head, (2) repair of the lateral ulnar collateral ligament, and (3) repair of the coronoid fracture. During the study period, the radial head generally was internally fixed when there were fewer than four articular fragments; otherwise, it was replaced. Evaluation included the DASH score, the Broberg-Morrey index, measurements of elbow stability and motion, and radiographic assessment for signs of arthrosis; chart review was performed for complications and reoperations. Complete followup was available on 87% (39 of 45 patients).
Results: There were no differences between groups in terms of ROM or elbow scores. All patients who underwent radial head arthroplasty at the index procedure had a stable elbow at final followup whereas three of nine patients who underwent ORIF were unstable (p = 0.009). However, 11 patients who underwent arthroplasty demonstrated radiographic signs of arthrosis compared to none in the ORIF group (p = 0.04). Eleven patients (28%) underwent reoperation (seven arthroplasty, four ORIF) for various reasons. With the numbers available, there was no difference in reoperation rate between groups (p = 0.45).
Conclusions: For terrible triad injuries, radial head arthroplasty afforded the ability to obtain elbow stability with comparable overall outcomes when compared to ORIF. As these injuries commonly occur in younger patients, longer-term studies will be required to ascertain whether the apparent benefits of radial head arthroplasty are offset by late complications of arthroplasty, such as loosening.
Level of evidence: Level III, therapeutic study. See the Instructions for Authors for a complete description of levels of evidence.
Figures

References
-
- Egol KA, Immerman I, Paksima N, Tejwani N, Koval KJ. Fracture-dislocation of the elbow functional outcome following treatment with a standardized protocol. Bull NYU Hosp Jt Dis. 2007;65:263–270. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
