

Risk factors and outcomes for late presentation for HIV-positive persons in Europe: results from the Collaboration of Observational HIV Epidemiological Research Europe Study (COHERE)
- PMID: 24137103
- PMCID: PMC3796947
- DOI: 10.1371/journal.pmed.1001510
Risk factors and outcomes for late presentation for HIV-positive persons in Europe: results from the Collaboration of Observational HIV Epidemiological Research Europe Study (COHERE)
Abstract
Background: Few studies have monitored late presentation (LP) of HIV infection over the European continent, including Eastern Europe. Study objectives were to explore the impact of LP on AIDS and mortality.
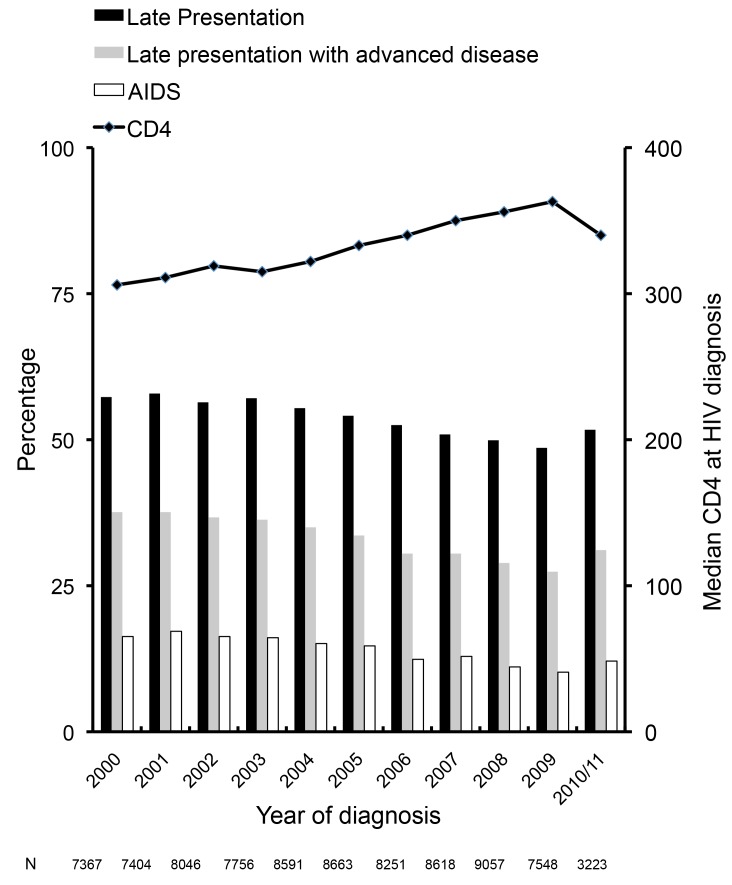
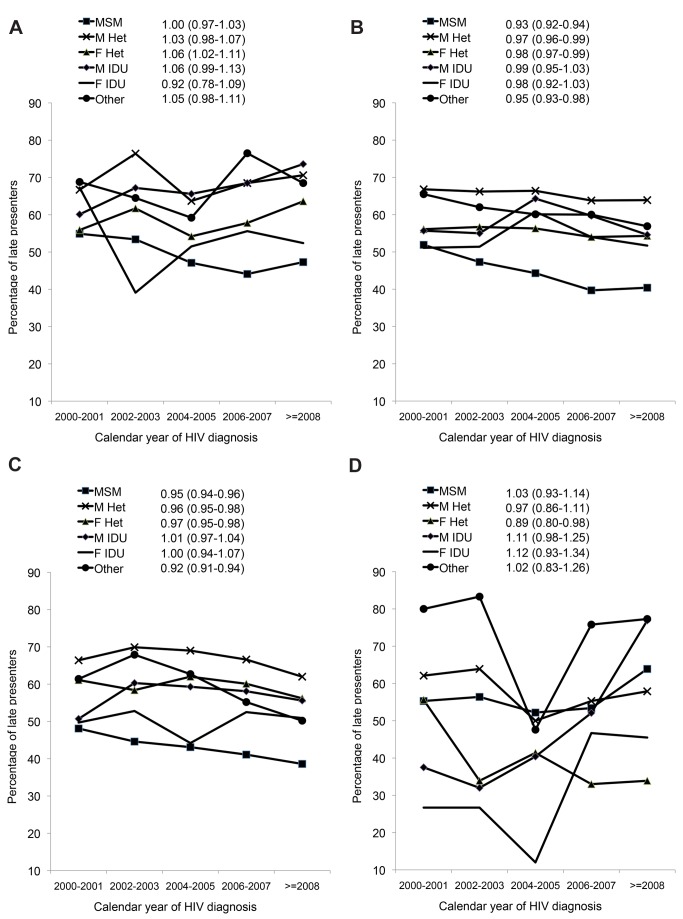
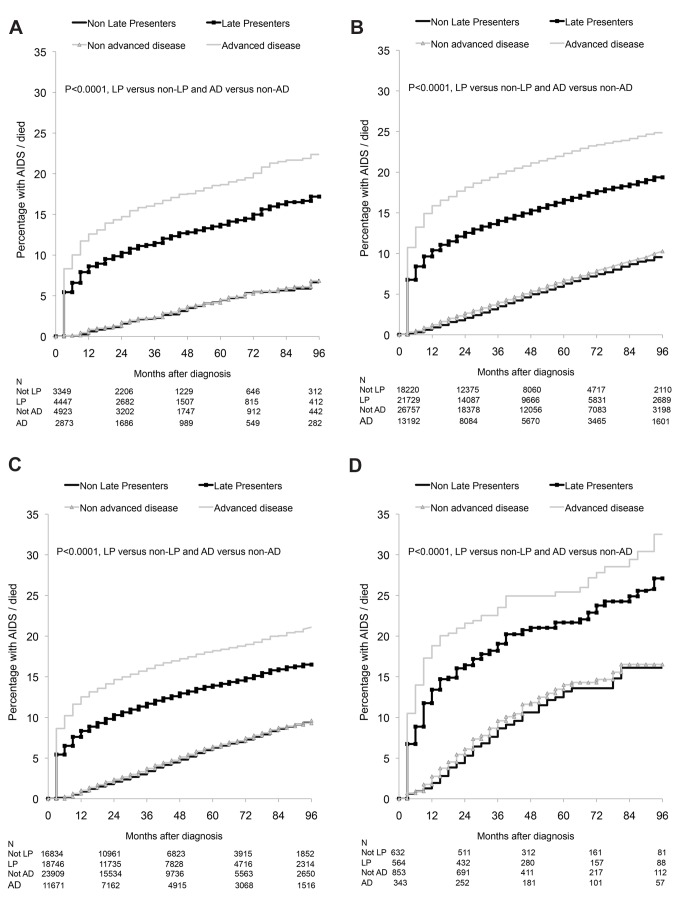
Methods and findings: LP was defined in Collaboration of Observational HIV Epidemiological Research Europe (COHERE) as HIV diagnosis with a CD4 count <350/mm(3) or an AIDS diagnosis within 6 months of HIV diagnosis among persons presenting for care between 1 January 2000 and 30 June 2011. Logistic regression was used to identify factors associated with LP and Poisson regression to explore the impact on AIDS/death. 84,524 individuals from 23 cohorts in 35 countries contributed data; 45,488 were LP (53.8%). LP was highest in heterosexual males (66.1%), Southern European countries (57.0%), and persons originating from Africa (65.1%). LP decreased from 57.3% in 2000 to 51.7% in 2010/2011 (adjusted odds ratio [aOR] 0.96; 95% CI 0.95-0.97). LP decreased over time in both Central and Northern Europe among homosexual men, and male and female heterosexuals, but increased over time for female heterosexuals and male intravenous drug users (IDUs) from Southern Europe and in male and female IDUs from Eastern Europe. 8,187 AIDS/deaths occurred during 327,003 person-years of follow-up. In the first year after HIV diagnosis, LP was associated with over a 13-fold increased incidence of AIDS/death in Southern Europe (adjusted incidence rate ratio [aIRR] 13.02; 95% CI 8.19-20.70) and over a 6-fold increased rate in Eastern Europe (aIRR 6.64; 95% CI 3.55-12.43).
Conclusions: LP has decreased over time across Europe, but remains a significant issue in the region in all HIV exposure groups. LP increased in male IDUs and female heterosexuals from Southern Europe and IDUs in Eastern Europe. LP was associated with an increased rate of AIDS/deaths, particularly in the first year after HIV diagnosis, with significant variation across Europe. Earlier and more widespread testing, timely referrals after testing positive, and improved retention in care strategies are required to further reduce the incidence of LP.
Conflict of interest statement
AM has received lecture fees, honoraria, and/or consultancies from Pfizer, BI, BMS, Merck, and Gilead. Ad'A is an advisory board member of BMS, Jannsen, Gilead, and ViiV. GF has received honoraria for lectures and advisory boards from Abbott, Bristol-Myers Squibb, Gilead, Janssen-Cilag, and Merck Sharp & Dohme. Research grant to GF from the German Federal Ministry of Education and Research (BMBF) 01KI1017. AJ is a Governor of the Wellcome Trust, a charitable research funding body; in 2011 was a specialist adviser to House of Lords Select Committee on HIV/AIDS; is a member of the UK Expert Advisory Group on AIDS; receives research grant funding from the UK Medical Research Council, Wellcome Trust, UK National Institute for Health Research, and Department of Health. CL has received these research grants: ANRS CMIT soutien (Aproco-Copilote ANRS CO08 HIV cohort, 1997–2012); IMMI (Cohort Fluco A(H1N1) pandemic influenza, 2009–2012); Ministère de la Santé PHRC (Bivir influenza trial, Oseltamivir Zanamivir, 2006–2012). CS has received funding for Advisory Board membership, speaker panels, and provision of educational materials for Gilead Sciences, Abbott Pharmaceuticals, ViiV, Merck Sharp & Dohme, Janssen-Cilag, and Bristol-Myers Squibb. CT has received honoraria to act as speaker at CME conferences on antiretroviral therapy and HIV disease management from several companies producing antiretroviral drugs, received travel grants to participate in scientific conferences, and acted as scientific consultant for the same companies. GC has had scientific responsibilities in projects receiving specific grant support from the French Agency for Research on AIDS and Viral Hepatitis (ANRS), the European Commission (Framework Program 7), UK Medical Research Council, US National Institute of Health (NIH), Fondation Plan Alzheimer, Gilead, Tibotec, Boehringer Ingelheim, GlaxoSmithKline, Roche, Pfizer, Merck, Abbott, Bristol-Myers Squibb, Janssen, ViiV Healthcare – these grants are managed through her Institution or a non-profit society. GC also serves as Academic Editor on PLOS ONE and is on the editorial board of the BMC Infectious Diseases Journal. OK has received honoraria, consultancy, lecture fees, and travel grants from Abbott Laboratories, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp & Dohme, Roche, and ViiV Healthcare, and has served/is serving on Advisory Boards for Gilead Sciences, Merck Sharp & Dohme, and ViiV Healthcare. No other competing interests have been declared.
Figures
References
-
- Girardi E, Aloisi MS, Arici C, Pezzotti P, Serraino D, et al. (2004) Delayed presentation and late testing for HIV: demographic and behavioral risk factors in a multicenter study in Italy. J Acquir Immune Defic Syndr 36: 951–959. - PubMed
-
- Antinori A, Coenen T, Costagiola D, Dedes N, Ellefson M, et al. (2011) Late presentation of HIV infection: a consensus definition. HIV Med 12: 61–64. - PubMed
-
- World Health Organization (2010) Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach.– 2010 revision. Available: http://whqlibdoc.who.int/publications/2010/9789241599764_eng.pdf. Accessed 23 July 2013. - PubMed
-
- Battegay M, Fluckiger U, Hirschel B, Furrer H (2007) Late presentation of HIV-infected individuals. Antivir Ther 12: 841–851. - PubMed
-
- Sabin CA, Smith CJ, Gumley H, Murphy G, Lampe FC, et al. (2004) Late presenters in the era of highly active antiretroviral therapy: uptake of and responses to antiretroviral therapy. AIDS 18: 2145–2151. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
