

Low-cost tele-assessment system for home-based evaluation of reaching ability following stroke
- PMID: 24138613
- PMCID: PMC3850429
- DOI: 10.1089/tmj.2012.0300
Low-cost tele-assessment system for home-based evaluation of reaching ability following stroke
Abstract
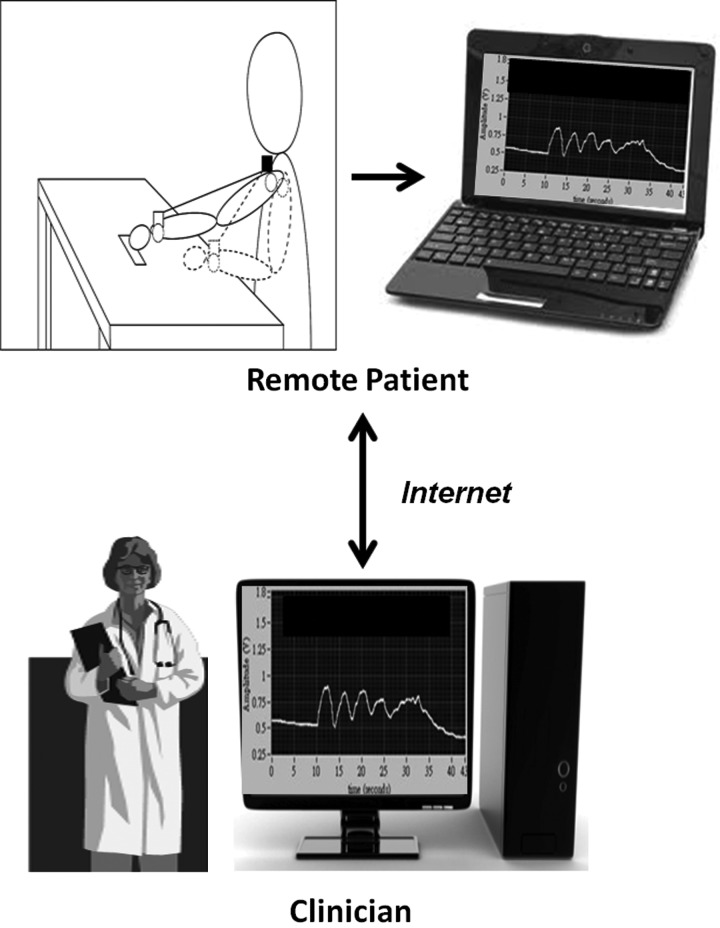
Objective: Tele-assessment techniques can provide healthcare professionals with easily accessible information regarding patients' clinical progress. Recently, kinematic analysis systems have been used to assess rehabilitative outcomes in stroke patients. Kinematic systems, however, are not compatible with tele-assessment. The objective of our study was to develop a tele-assessment system for acquiring kinematic data of forward reaching movements in stroke patients, with an emphasis on cost-effectiveness, portability, and ease of use.
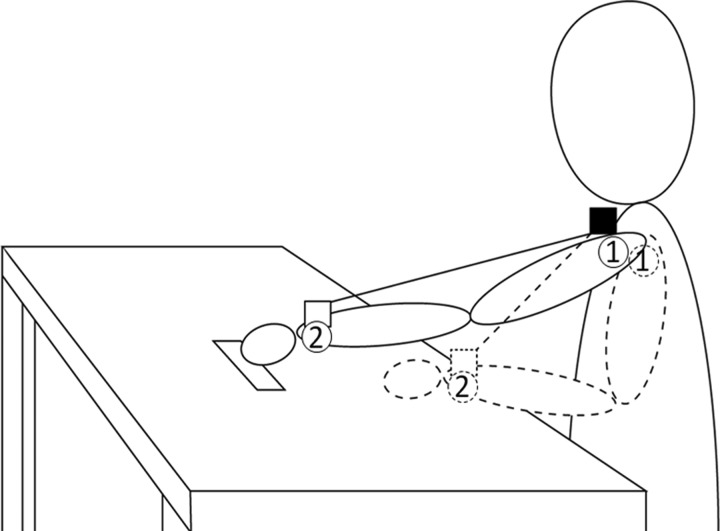
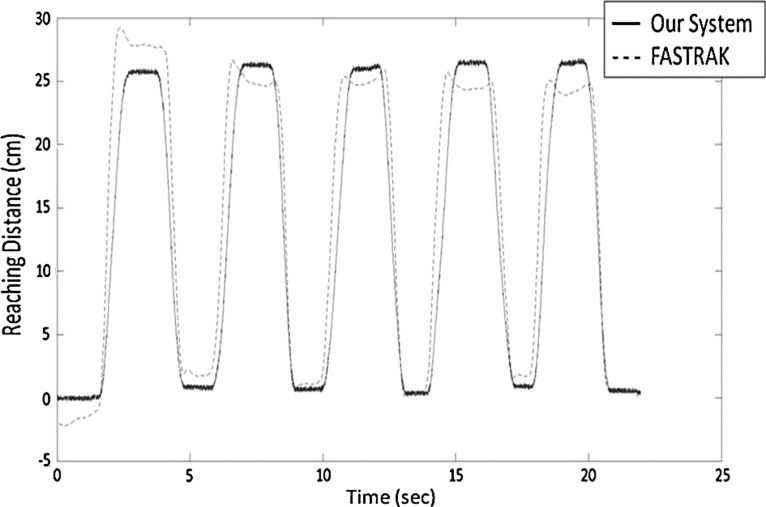
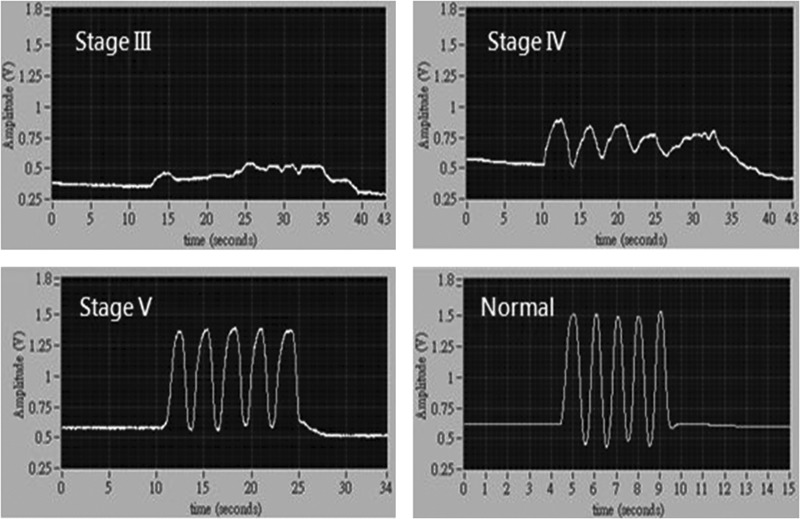
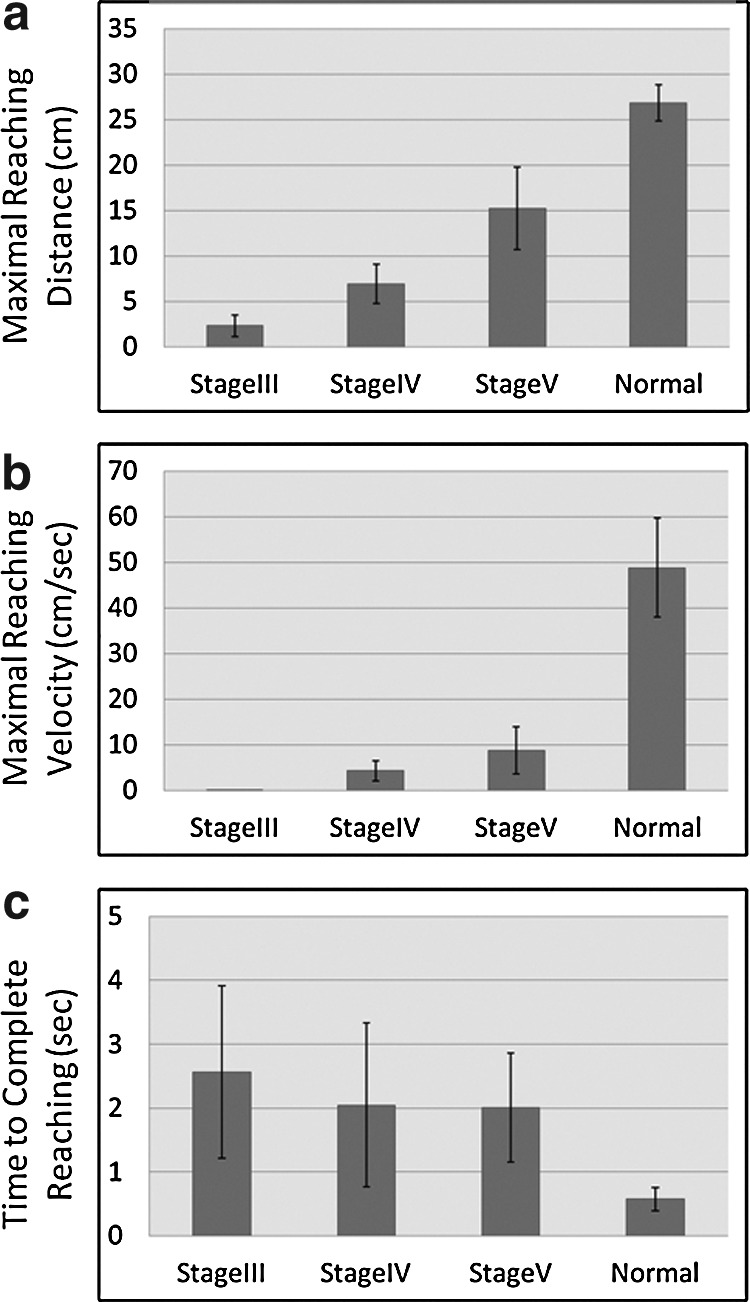
Materials and methods: We selected four healthy control participants and eight hemiplegic stroke patients for our study. The stroke patients were classified as Brunnstrom stage III, stage IV, or stage V. Our tele-assessment system used two three-axes accelerometers, a potentiometer, a multifunctional data acquisition card, and two computers. A standardized kinematic system was applied simultaneously to validate the measurements recorded by our tele-assessment system during five repetitions of forward reaching movements.
Results: The correlation coefficients of the reaching displacement, velocity, and acceleration measurements obtained using our tele-assessment system and the standardized kinematic system were 0.956, 0.896, and 0.727, respectively. Differences in the maximum reaching distance and the maximum reaching velocity of forward reaching movements were observed among the study groups. There were no significant differences in the time required to complete the testing session among the study groups.
Conclusions: Our tele-assessment system is valid for the evaluation of upper-extremity reaching ability in stroke patients. Further research is needed to investigate the feasibility of the use of the tele-assessment system in patients' homes.
Figures
Similar articles
-
Cost analysis of in-home telerehabilitation for post-knee arthroplasty.J Med Internet Res. 2015 Mar 31;17(3):e83. doi: 10.2196/jmir.3844. J Med Internet Res. 2015. PMID: 25840501 Free PMC article. Clinical Trial.
-
Motor tele-rehabilitation in post-stroke patients.Med Inform Internet Med. 2004 Jun;29(2):119-25. doi: 10.1080/14639230410001723428. Med Inform Internet Med. 2004. PMID: 15370992
-
Toward a low-cost, in-home, telemedicine-enabled assessment of disability in multiple sclerosis.Mult Scler. 2019 Oct;25(11):1526-1534. doi: 10.1177/1352458518793527. Epub 2018 Aug 24. Mult Scler. 2019. PMID: 30141729
-
Clinical and Economic Outcomes of Telemedicine Programs in the Intensive Care Unit: A Systematic Review and Meta-Analysis.J Intensive Care Med. 2018 Jul;33(7):383-393. doi: 10.1177/0885066617726942. Epub 2017 Aug 22. J Intensive Care Med. 2018. PMID: 28826282
-
Systematic Review on Kinematic Assessments of Upper Limb Movements After Stroke.Stroke. 2019 Mar;50(3):718-727. doi: 10.1161/STROKEAHA.118.023531. Stroke. 2019. PMID: 30776997
Cited by
-
Digital Technology Enablers of Tele-Neurorehabilitation in Pre- and Post-COVID-19 Pandemic Era - A Scoping Review.Int J Telerehabil. 2024 Jun 28;16(1):e6611. doi: 10.5195/ijt.2024.6611. eCollection 2024. Int J Telerehabil. 2024. PMID: 39022438 Free PMC article.
-
Remotely Assessing Motor Function and Activity of the Upper Extremity After Stroke: A Systematic Review of Validity and Clinical Utility of Tele-Assessments.Clin Rehabil. 2024 Sep;38(9):1214-1225. doi: 10.1177/02692155241258867. Epub 2024 Jun 5. Clin Rehabil. 2024. PMID: 38839104 Free PMC article.
-
Clinical Study of a Wearable Remote Rehabilitation Training System for Patients With Stroke: Randomized Controlled Pilot Trial.JMIR Mhealth Uhealth. 2023 Feb 23;11:e40416. doi: 10.2196/40416. JMIR Mhealth Uhealth. 2023. PMID: 36821348 Free PMC article. Clinical Trial.
-
Intra- and Interrater Reliability of Remote Assessment of Transfers by Wheelchair Users Using the Transfer Assessment Instrument (Version 4.0).Arch Phys Med Rehabil. 2022 Apr;103(4):816-821. doi: 10.1016/j.apmr.2020.12.032. Epub 2021 Mar 10. Arch Phys Med Rehabil. 2022. PMID: 33711281 Free PMC article.
-
Teleassessment of Gait and Gait Aids: Validity and Interrater Reliability.Phys Ther. 2020 Apr 17;100(4):708-717. doi: 10.1093/ptj/pzaa005. Phys Ther. 2020. PMID: 31984420 Free PMC article.
References
-
- Ytterberg C. Thorsén A-M. Liljedahl M, et al. Changes in perceived health between one and five years after stroke: A randomized controlled trial of early supported discharge with continued rehabilitation at home versus conventional rehabilitation. J Neurol Sci. 2010;294:86–88. - PubMed
-
- Johansson T. Wild C. Telerehabilitation in stroke care—A systematic review. J Telemed Telecare. 2011;17:1–6. - PubMed
-
- Piron L. Turolla A. Agostini M, et al. Exercises for paretic upper limb after stroke: A combined virtual-reality and telemedicine approach. J Rehabil Med. 2009;41:1016–1102. - PubMed
-
- Piron L. Tonin P. Trivello E, et al. Motor tele-rehabilitation in post-stroke patients. Med Inform Internet Med. 2004;29:119–125. - PubMed
-
- Holden MK. Dyar TA. Dayan-Cimadoro L. Telerehabilitation using a virtual environment improves upper extremity function in patients with stroke. IEEE Trans Neural Syst Rehabil Eng. 2007;15:36–42. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
