

Fluid balance and cardiac function in septic shock as predictors of hospital mortality
- PMID: 24138869
- PMCID: PMC4056694
- DOI: 10.1186/cc13072
Fluid balance and cardiac function in septic shock as predictors of hospital mortality
Abstract
Introduction: Septic shock is a major cause of morbidity and mortality throughout the world. Unfortunately, the optimal fluid management of septic shock is unknown and currently is empirical.
Methods: A retrospective analysis was performed at Barnes-Jewish Hospital (St. Louis, Missouri). Consecutive patients (n = 325) hospitalized with septic shock who had echocardiographic examinations performed within 24 hours of shock onset were enrolled.
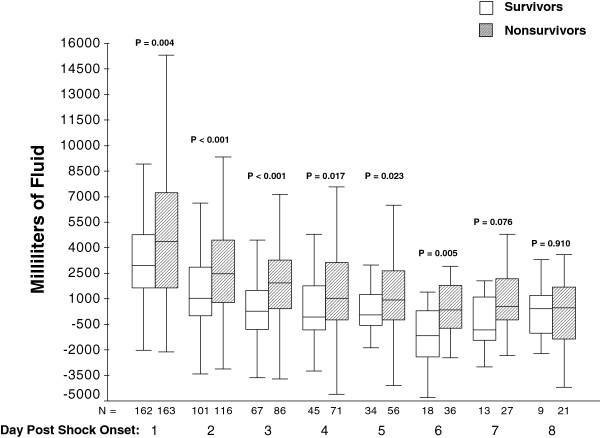
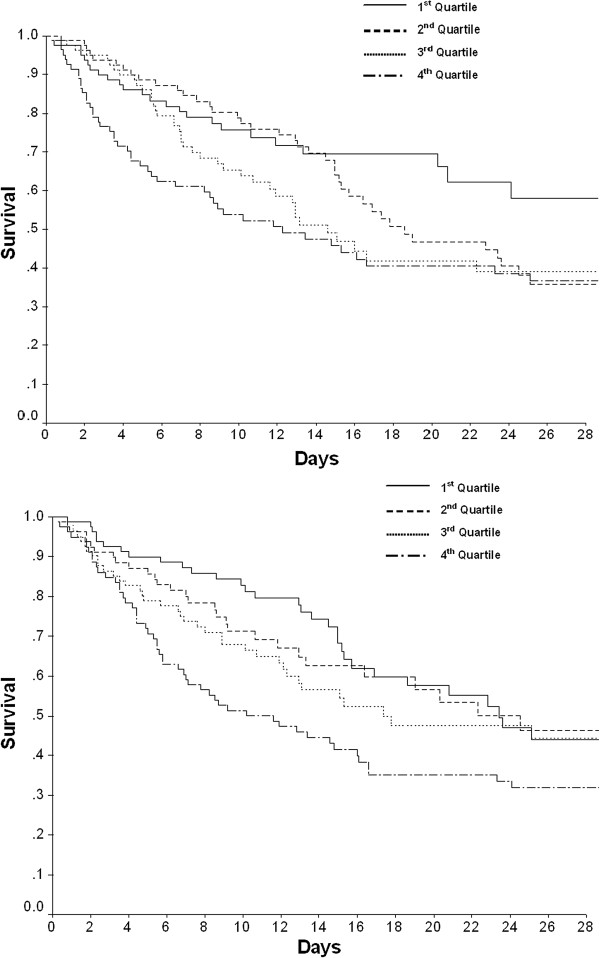
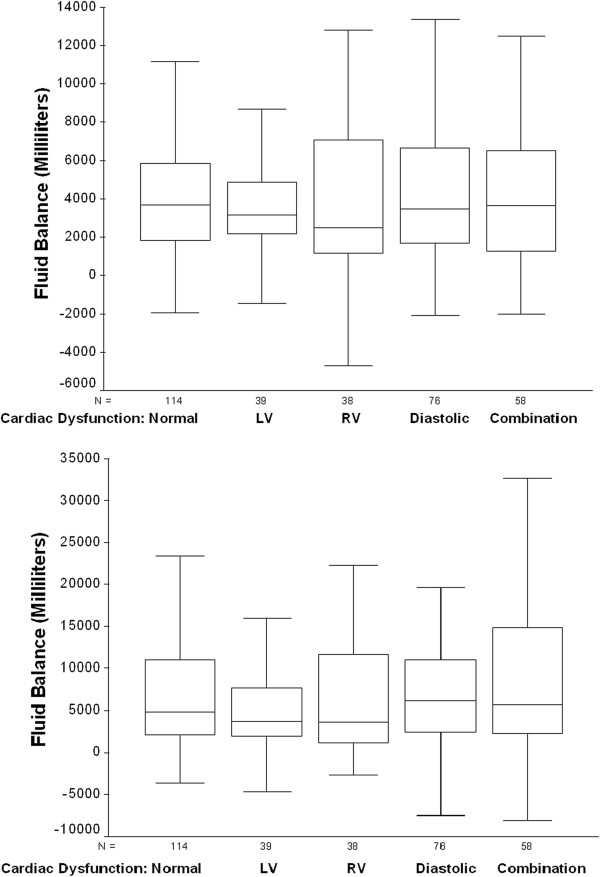
Results: A total of 163 (50.2%) patients with septic shock died during hospitalization. Non-survivors had a significantly larger positive net fluid balance within the 24 hour window of septic shock onset (median (IQR): 4,374 ml (1,637 ml, 7,260 ml) vs. 2,959 ml (1,639.5 ml, 4,769.5 ml), P = 0.004). The greatest quartile of positive net fluid balance at 24 hours and eight days post-shock onset respectively were found to predict hospital mortality, and the greatest quartile of positive net fluid balance at eight days post-shock onset was an independent predictor of hospital mortality (adjusted odds ratio (AOR), 1.66; 95% CI, 1.39 to 1.98; P = 0.004). Survivors were significantly more likely to have mild left ventricular dysfunction as evaluated by bedside echocardiography and non-survivors had slightly elevated left ventricular ejection fraction, which was also found to be an independent predictor of outcome.
Conclusions: Our data confirms the importance of fluid balance and cardiac function as outcome predictors in patients with septic shock. A clinical trial to determine the optimal administration of intravenous fluids to patients with septic shock is needed.
Figures
References
-
- Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL. International Surviving Sepsis Campaign Guidelines Committee, American Association of Critical-Care Nurses, American College of Chest Physicians, American College of Emergency Physicians, Canadian Critical Care Society, European Society of Clinical Microbiology and Infectious Diseases et al.Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;17:296–327. doi: 10.1097/01.CCM.0000298158.12101.41. - DOI - PubMed
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb SA, Beale RJ, Vincent JL, Moreno R. Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;17:580–637. doi: 10.1097/CCM.0b013e31827e83af. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
