

Alterations in brain structure and neurodevelopmental outcome in preterm infants hospitalized in different neonatal intensive care unit environments
- PMID: 24139564
- PMCID: PMC3872171
- DOI: 10.1016/j.jpeds.2013.08.047
Alterations in brain structure and neurodevelopmental outcome in preterm infants hospitalized in different neonatal intensive care unit environments
Erratum in
- J Pediatr. 2015 Apr;166(4):1097
Abstract
Objective: To evaluate associations between neonatal intensive care unit (NICU) room type (open ward and private room) and medical outcomes; neurobehavior, electrophysiology, and brain structure at hospital discharge; and developmental outcomes at 2 years of age.
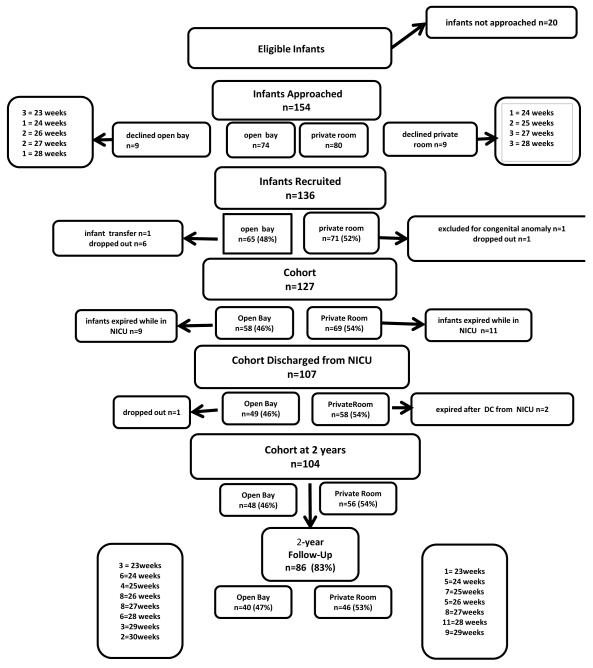
Study design: In this prospective longitudinal cohort study, we enrolled 136 preterm infants born <30 weeks gestation from an urban, 75-bed level III NICU from 2007-2010. Upon admission, each participant was assigned to a bedspace in an open ward or private room within the same hospital, based on space and staffing availability, where they remained for the duration of hospitalization. The primary outcome was developmental performance at 2 years of age (n = 86 infants returned for testing, which was 83% of survivors) measured using the Bayley Scales of Infant and Toddler Development, 3rd Edition. Secondary outcomes were: (1) medical factors throughout the hospitalization; (2) neurobehavior; and (3) cerebral injury and maturation (determined by magnetic resonance imaging and electroencephalography).
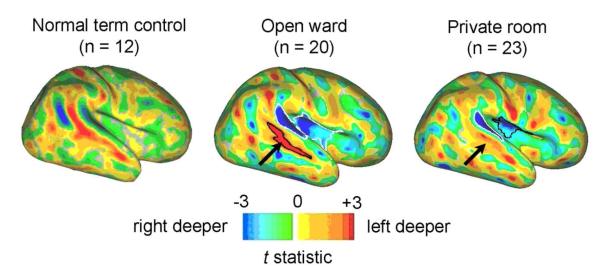
Results: At term equivalent age, infants in private rooms were characterized by a diminution of normal hemispheric asymmetry and a trend toward having lower amplitude integrated electroencephalography cerebral maturation scores (P = .02; β = -0.52 [CI -0.95, -0.10]). At age 2 years, infants from private rooms had lower language scores (P = .006; β = -8.3 [CI -14.2, -2.4]) and a trend toward lower motor scores (P = .02; β = -6.3 [CI -11.7, -0.99]), which persisted after adjustment for potential confounders.
Conclusion: These findings raise concerns that highlight the need for further research into the potential adverse effects of different amounts of sensory exposure in the NICU environment.
Keywords: Amplitude integrated electroencephalography; Bayley Scales of Infant and Toddler Development, 3rd edition; Bayley-III; CRIB; Critical Risk Index for Babies; Echo time; FA; FAD; Fractional anisotropy; Functional connectivity magnetic resonance imaging; ITSEA; Infant Toddler Social Emotional Assessment; M-CHAT; MRI; Magnetic resonance imaging; McMaster Family Assessment Device; Modified Checklist for Autism in Toddlers; NICU; NICU Network Neurobehavioral Scale; NNNS; Neonatal intensive care unit; PDA; PMA; Patent ductus arteriosus; Postmenstrual age; Repetition time; TE; TR; aEEG; fcMRI.
Copyright © 2014 Mosby, Inc. All rights reserved.
Figures
References
-
- Lasky RE, Williams AL. Noise and light exposures for extremely low birth weight newborns during their stay in the neonatal intensive care unit. Pediatrics. 2009;123:540–6. - PubMed
-
- Noise: a hazard for the fetus and newborn. American Academy of Pediatrics. Committee on Environmental Health. Pediatrics. 1997;100:724–7. - PubMed
-
- Liu WF, Laudert S, Perkins B, Macmillan-York E, Martin S, Graven S. The development of potentially better practices to support the neurodevelopment of infants in the NICU. Journal of perinatology : official journal of the California Perinatal Association. 2007;27(Suppl 2):S48–74. - PubMed
-
- Hassanein SM, El Raggal NM, Shalaby AA. Neonatal nursery noise: practice-based learning and improvement. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstet. 2012 - PubMed
-
- Als H, Brazelton TB. A new model of assessing the behavioral organization in preterm and fullterm infants: two case studies. Journal of the American Academy of Child Psychiatry. 1981;20:239–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
