

Recurrence patterns across medulloblastoma subgroups: an integrated clinical and molecular analysis
- PMID: 24140199
- PMCID: PMC3953419
- DOI: 10.1016/S1470-2045(13)70449-2
Recurrence patterns across medulloblastoma subgroups: an integrated clinical and molecular analysis
Erratum in
- Lancet Oncol. 2014 Apr;15(4):e154
Abstract
Background: Recurrent medulloblastoma is a therapeutic challenge because it is almost always fatal. Studies have confirmed that medulloblastoma consists of at least four distinct subgroups. We sought to delineate subgroup-specific differences in medulloblastoma recurrence patterns.
Methods: We retrospectively identified a discovery cohort of all recurrent medulloblastomas at the Hospital for Sick Children (Toronto, ON, Canada) from 1994 to 2012 (cohort 1), and established molecular subgroups using a nanoString-based assay on formalin-fixed paraffin-embedded tissues or frozen tissue. The anatomical site of recurrence (local tumour bed or leptomeningeal metastasis), time to recurrence, and survival after recurrence were assessed in a subgroup-specific manner. Two independent, non-overlapping cohorts (cohort 2: samples from patients with recurrent medulloblastomas from 13 centres worldwide, obtained between 1991 and 2012; cohort 3: samples from patients with recurrent medulloblastoma obtained at the NN Burdenko Neurosurgical Institute [Moscow, Russia] between 1994 and 2011) were analysed to confirm and validate observations. When possible, molecular subgrouping was done on tissue obtained from both the initial surgery and at recurrence.
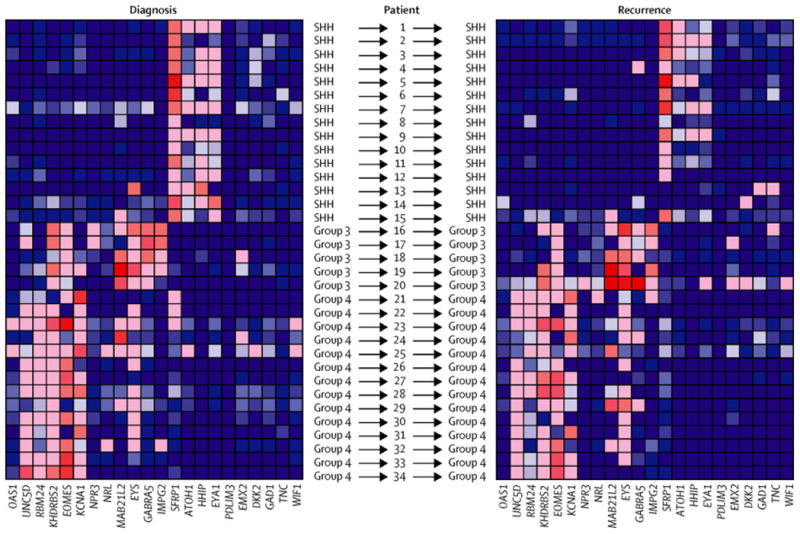
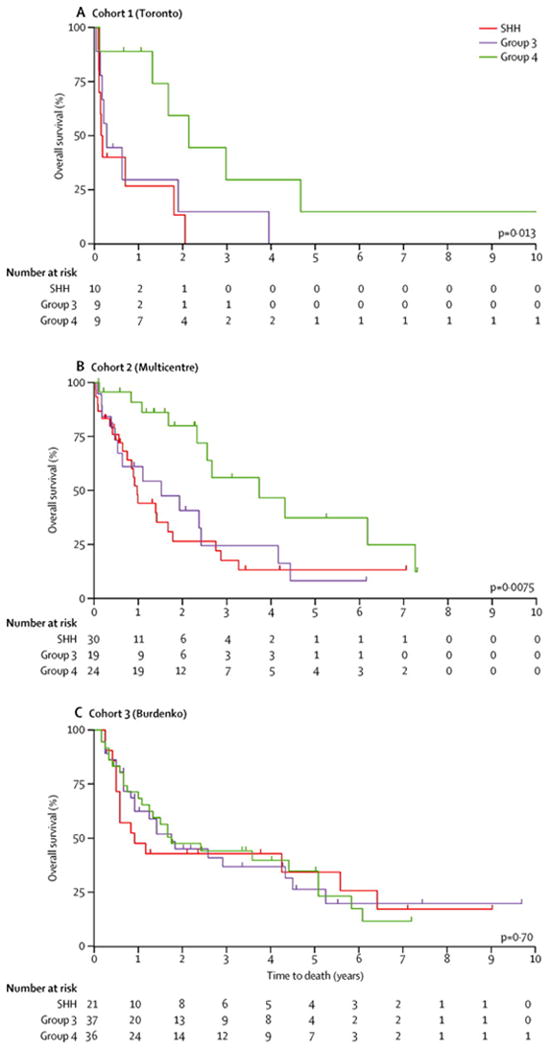
Results: Cohort 1 consisted of 30 patients with recurrent medulloblastomas; nine with local recurrences, and 21 with metastatic recurrences. Cohort 2 consisted of 77 patients and cohort 3 of 96 patients with recurrent medulloblastoma. Subgroup affiliation remained stable at recurrence in all 34 cases with available matched primary and recurrent pairs (five pairs from cohort 1 and 29 pairs from cohort 2 [15 SHH, five group 3, 14 group 4]). This finding was validated in 17 pairs from cohort 3. When analysed in a subgroup-specific manner, local recurrences in cohort 1 were more frequent in SHH tumours (eight of nine [89%]) and metastatic recurrences were more common in group 3 and group 4 tumours (17 of 20 [85%] with one WNT, p=0·0014, local vs metastatic recurrence, SHH vs group 3 vs group 4). The subgroup-specific location of recurrence was confirmed in cohort 2 (p=0·0013 for local vs metastatic recurrence, SHH vs group 3 vs group 4,), and cohort 3 (p<0·0001). Treatment with craniospinal irradiation at diagnosis was not significantly associated with the anatomical pattern of recurrence. Survival after recurrence was significantly longer in patients with group 4 tumours in cohort 1 (p=0·013) than with other subgroups, which was confirmed in cohort 2 (p=0·0075), but not cohort 3 (p=0·70).
Interpretation: Medulloblastoma does not change subgroup at the time of recurrence, reinforcing the stability of the four main medulloblastoma subgroups. Significant differences in the location and timing of recurrence across medulloblastoma subgroups have potential treatment ramifications. Specifically, intensified local (posterior fossa) therapy should be tested in the initial treatment of patients with SHH tumours. Refinement of therapy for patients with group 3 or group 4 tumours should focus on metastases.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of Interests: The authors declare no conflicts of interest.
Figures
Comment in
-
Genetics of recurrent medulloblastoma.Lancet Oncol. 2013 Nov;14(12):1147-8. doi: 10.1016/S1470-2045(13)70482-0. Epub 2013 Oct 17. Lancet Oncol. 2013. PMID: 24140202 No abstract available.
-
Neuro-oncology: Stability of medulloblastoma subgroups at tumour recurrence.Nat Rev Neurol. 2014 Jan;10(1):5-6. doi: 10.1038/nrneurol.2013.256. Epub 2013 Dec 10. Nat Rev Neurol. 2014. PMID: 24323052 No abstract available.
References
-
- Ramaswamy V, Northcott PA, Taylor MD. FISH and chips: the recipe for improved prognostication and outcomes for children with medulloblastoma. Cancer genetics. 2011;204(11):577–88. - PubMed
-
- Packer RJ, Gajjar A, Vezina G, et al. Phase III study of craniospinal radiation therapy followed by adjuvant chemotherapy for newly diagnosed average-risk medulloblastoma. J Clin Oncol. 2006;24(25):4202–8. - PubMed
-
- Gajjar A, Chintagumpala M, Ashley D, et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): long-term results from a prospective, multicentre trial. Lancet Oncol. 2006;7(10):813–20. - PubMed
-
- Tarbell NJ, Friedman H, Polkinghorn WR, et al. High-Risk Medulloblastoma: A Pediatric Oncology Group Randomized Trial of Chemotherapy Before or After Radiation Therapy (POG 9031) Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2013;31(23):2936–41. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
