

Dyslipidemia, coronary artery calcium, and incident atherosclerotic cardiovascular disease: implications for statin therapy from the multi-ethnic study of atherosclerosis
- PMID: 24141324
- PMCID: PMC3919521
- DOI: 10.1161/CIRCULATIONAHA.113.003625
Dyslipidemia, coronary artery calcium, and incident atherosclerotic cardiovascular disease: implications for statin therapy from the multi-ethnic study of atherosclerosis
Abstract
Background: Worldwide clinical practice guidelines for dyslipidemia emphasize allocating statin therapy to those at the highest absolute atherosclerotic cardiovascular disease (CVD) risk.
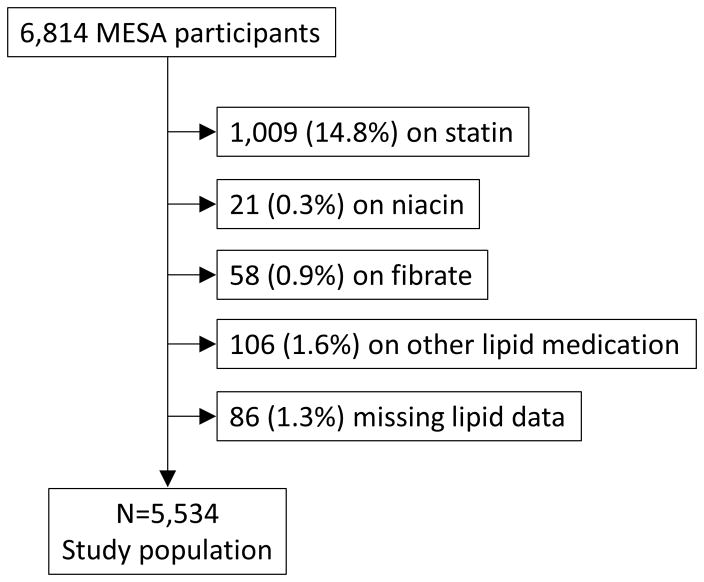
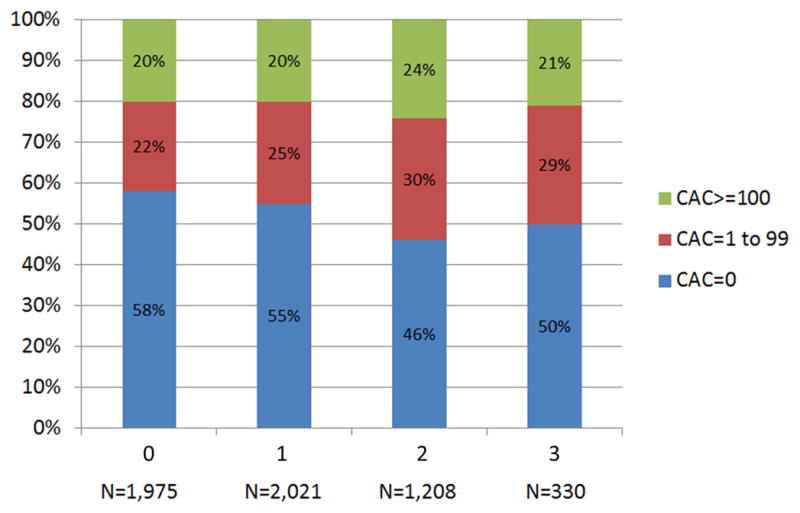
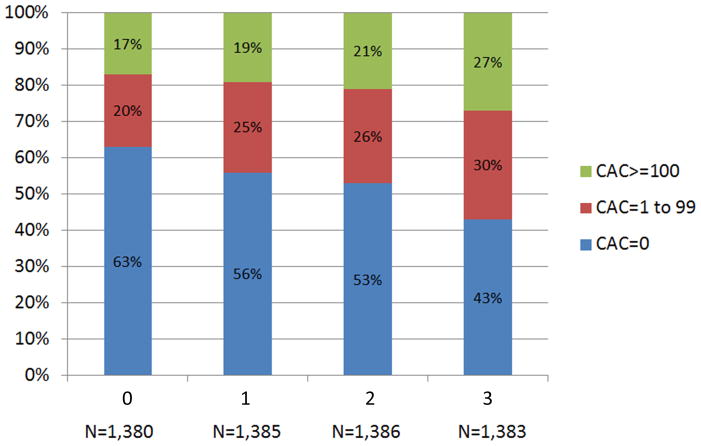
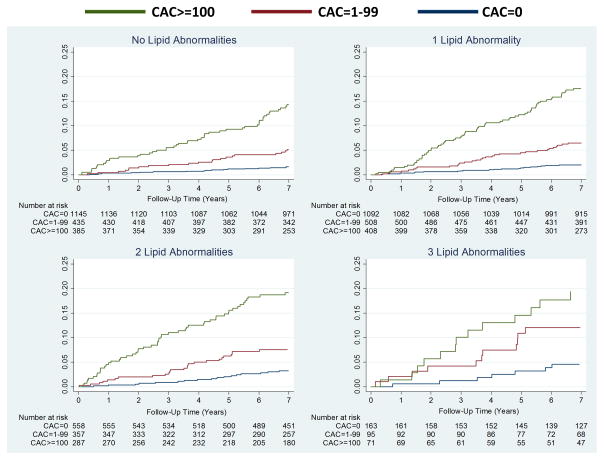
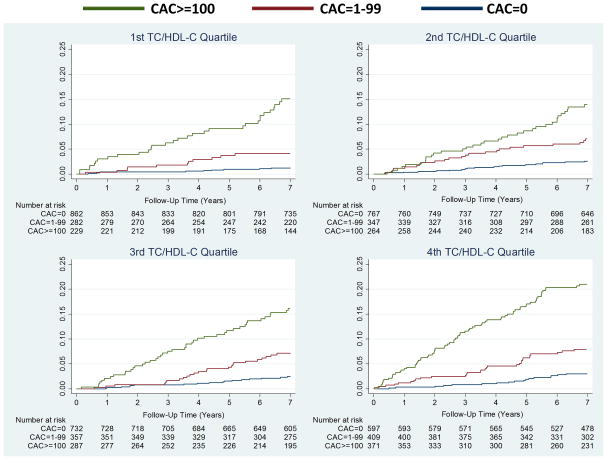
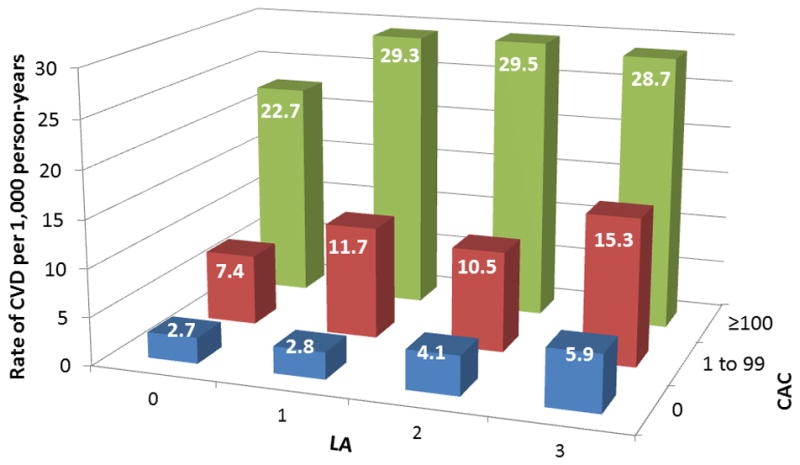
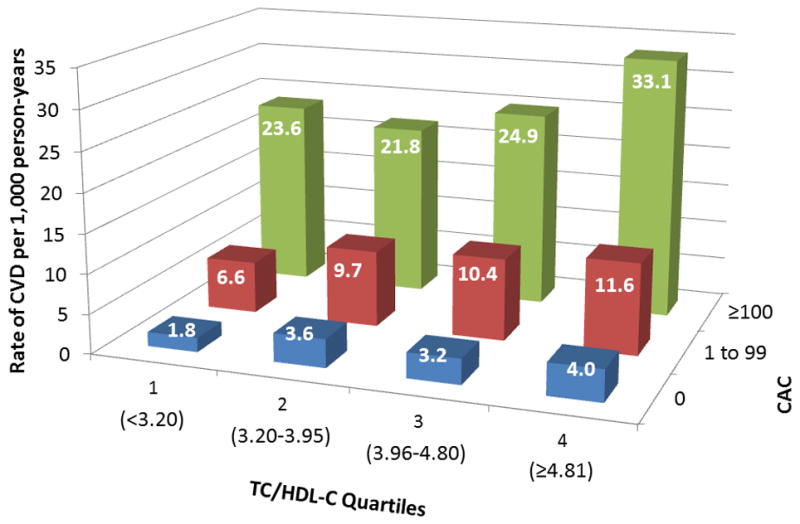
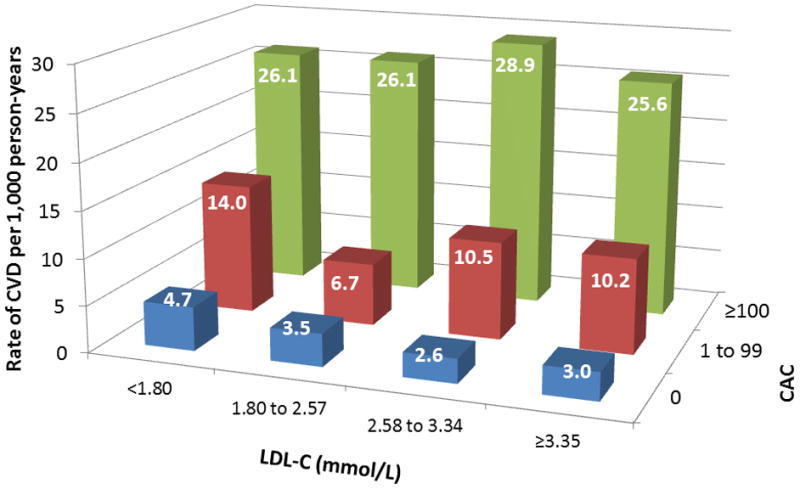
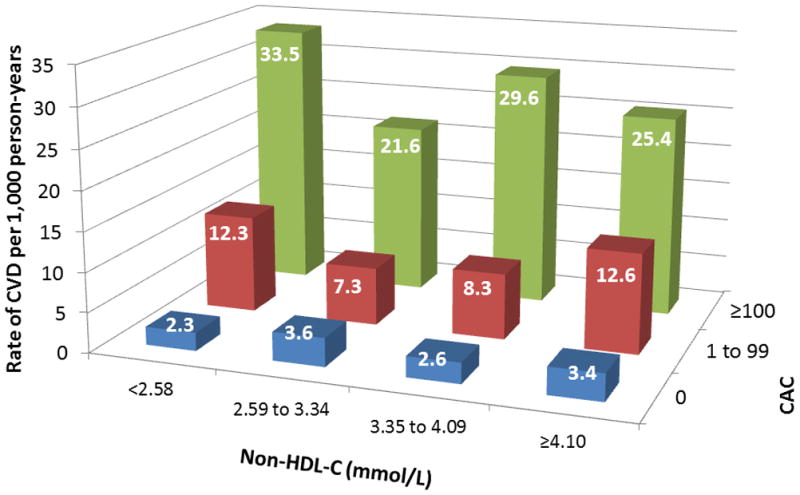
Methods and results: We examined 5534 Multi-Ethnic Study of Atherosclerosis (MESA) participants who were not on baseline medications for dyslipidemia. Participants were classified by baseline coronary artery calcium (CAC) score (>0, ≥ 100) and the common clinical scheme of counting lipid abnormalities (LA), including low-density lipoprotein cholesterol ≥ 3.36 mmol/L (130 mg/dL), high-density lipoprotein cholesterol <1.03 mmol/L (40 mg/dL) for men or <1.29 mmol/L (50 mg/dL) for women, and triglycerides ≥ 1.69 mmol/L (150 mg/dL). Our main outcome measure was incident CVD (myocardial infarction, angina resulting in revascularization, resuscitated cardiac arrest, stroke, cardiovascular death). Over a median follow-up of 7.6 years, more than half of events (55%) occurred in the 21% of participants with CAC ≥ 100. Conversely, 65% of events occurred in participants with 0 or 1 LA. In those with CAC ≥ 100, CVD rates ranged from 22.7 to 29.5 per 1000 person-years across LA categories. In contrast, with CAC=0, CVD rates ranged from 2.7 to 5.9 per 1000 person-years across LA categories. Individuals with 0 LA and CAC ≥ 100 had a higher event rate compared with individuals with 3 LA but CAC=0 (22.7 versus 5.9 per 1000 person-years). Similar results were obtained when we classified LA using data set quartiles of total cholesterol/high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, non-high-density lipoprotein cholesterol, or low-density lipoprotein particle concentration and guideline categories of low-density lipoprotein cholesterol or non-high-density lipoprotein cholesterol.
Conclusions: CAC may have the potential to help match statin therapy to absolute CVD risk. Across the spectrum of dyslipidemia, event rates similar to secondary prevention populations were observed for patients with CAC ≥ 100.
Keywords: atherosclerosis; cardiovascular diseases; cholesterol; computed tomography.
Conflict of interest statement
Figures
References
-
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Circulation. 2002;106:3143–421. - PubMed
-
- Grundy SM, Cleeman JI, Merz CN, Brewer HB, Jr, Clark LT, Hunninghake DB, Pasternak RC, Smith SC, Jr, Stone NJ. Coordinating Committee of the National Cholesterol Education Program. Circulation. 2004;110:227–39. - PubMed
-
- Reiner Z, Catapano AL, De Backer G, Graham I, Taskinen MR, Wiklund O, Agewall S, Alegria E, Chapman MJ, Durrington P, Erdine S, Halcox J, Hobbs R, Kjekshus J, Filardi PP, Riccardi G, Storey RF, Wood D European Association for Cardiovascular Prevention & Rehabilitation. ESC Committee for Practice Guidelines (CPG) 2008–2010 and 2010–2012 Committees. ESC/EAS Guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS) Eur Heart J. 2011;32:1769–1818. - PubMed
-
- Genest J, McPherson R, Frohlich J, Anderson T, Campbell N, Carpentier A, Couture P, Dufour R, Fodor G, Francis GA, Grover S, Gupta M, Hegele RA, Lau DC, Leiter L, Lewis GF, Lonn E, Mancini GB, Ng D, Pearson GJ, Sniderman A, Stone JA, Ur E, Genest J, McPherson R, Frohlich J. 2009 Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult - 2009 recommendations. Can J Cardiol. 2009;25:567–79. - PMC - PubMed
-
- Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, Peto R, Barnes EH, Keech A, Simes J, Collins R Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–81. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
