

Endoscopic treatments of endoscopic retrograde cholangiopancreatography-related duodenal perforations
- PMID: 24143315
- PMCID: PMC3797938
- DOI: 10.5946/ce.2013.46.5.522
Endoscopic treatments of endoscopic retrograde cholangiopancreatography-related duodenal perforations
Abstract
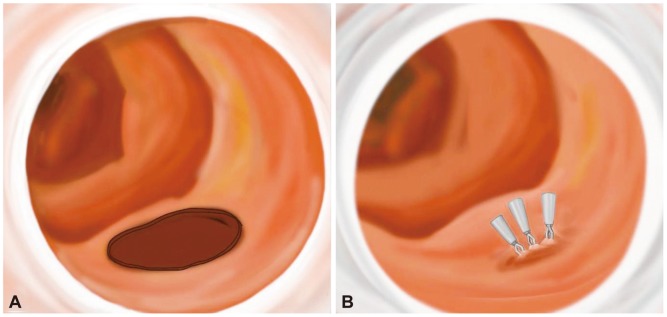
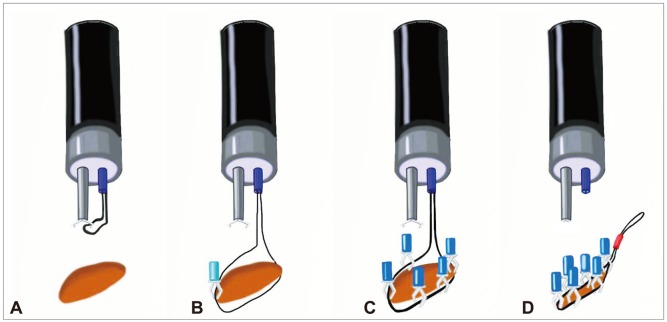
Iatrogenic duodenal perforation associated with endoscopic retrograde cholangiopancreatography (ERCP) is a very uncommon complication that is often lethal. Perforations during ERCP are caused by endoscopic sphincterotomy, placement of biliary or duodenal stents, guidewire-related causes, and endoscopy itself. In particular, perforation of the medial or lateral duodenal wall usually requires prompt diagnosis and surgical management. Perforation can follow various clinical courses, and management depends on the cause of the perforation. Cases resulting from sphincterotomy or guidewire-induced perforation can be managed by conservative treatment and biliary diversion. The current standard treatment for perforation of the duodenal free wall is early surgical repair. However, several reports of primary endoscopic closure techniques using endoclip, endoloop, or newly developed endoscopic devices have recently been described, even for use in direct perforation of the duodenal wall.
Keywords: Cholangiopancreatography, endoscopic retrograde; Duodenum; Perforation; Therapeutics.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures




Similar articles
-
Recent Advanced Endoscopic Management of Endoscopic Retrograde Cholangiopancreatography Related Duodenal Perforations.Clin Endosc. 2016 Jul;49(4):376-82. doi: 10.5946/ce.2016.088. Epub 2016 Jul 29. Clin Endosc. 2016. PMID: 27484814 Free PMC article. Review.
-
Primary endoscopic approximation suture under cap-assisted endoscopy of an ERCP-induced duodenal perforation.World J Gastroenterol. 2010 May 14;16(18):2305-10. doi: 10.3748/wjg.v16.i18.2305. World J Gastroenterol. 2010. PMID: 20458771 Free PMC article.
-
Closure of a persistent sphincterotomy-related duodenal perforation by placement of a covered self-expandable metallic biliary stent.World J Gastroenterol. 2011 Oct 28;17(40):4539-41. doi: 10.3748/wjg.v17.i40.4539. World J Gastroenterol. 2011. PMID: 22110286 Free PMC article.
-
Endoscopic Treatment of Endoscopic Retrograde Cholangiopancreatography-Related Duodenal Perforations.J Laparoendosc Adv Surg Tech A. 2019 Mar;29(3):385-391. doi: 10.1089/lap.2018.0617. Epub 2019 Jan 24. J Laparoendosc Adv Surg Tech A. 2019. Retraction in: J Laparoendosc Adv Surg Tech A. 2019 Jul;29(7):987. doi: 10.1089/lap.2018.0617.retract. PMID: 30676226 Retracted.
-
The management of endoscopic retrograde cholangiopancreatography-related duodenal perforation.Clin Endosc. 2014 Jul;47(4):341-5. doi: 10.5946/ce.2014.47.4.341. Epub 2014 Jul 28. Clin Endosc. 2014. PMID: 25133122 Free PMC article. Review.
Cited by
-
Endoscopic nasobiliary drainage tube placement through a periampullary perforation for management of intestinal leak and necrotizing pancreatitis.VideoGIE. 2022 Nov 21;8(2):75-77. doi: 10.1016/j.vgie.2022.09.004. eCollection 2023 Feb. VideoGIE. 2022. PMID: 36820259 Free PMC article.
-
Endoscopic Closure of an Acute Duodenal Perforation Occurring during Endoscopic Ultrasound Using Endoclips and Polyglycolic Acid Sheets with Fibrin Glue.Case Rep Gastroenterol. 2021 Mar 1;15(1):253-261. doi: 10.1159/000512474. eCollection 2021 Jan-Apr. Case Rep Gastroenterol. 2021. PMID: 33790712 Free PMC article.
-
Recent Advanced Endoscopic Management of Endoscopic Retrograde Cholangiopancreatography Related Duodenal Perforations.Clin Endosc. 2016 Jul;49(4):376-82. doi: 10.5946/ce.2016.088. Epub 2016 Jul 29. Clin Endosc. 2016. PMID: 27484814 Free PMC article. Review.
-
Post-endoscopic Retrograde Cholangiopancreatography Complications: A Case of Duodenal Perforation and Literature Review.Cureus. 2023 Jun 12;15(6):e40303. doi: 10.7759/cureus.40303. eCollection 2023 Jun. Cureus. 2023. PMID: 37313285 Free PMC article.
-
Value of temporary stents for the management of perivaterian perforation during endoscopic retrograde cholangiopancreatography.World J Clin Cases. 2014 Nov 16;2(11):689-97. doi: 10.12998/wjcc.v2.i11.689. World J Clin Cases. 2014. PMID: 25405193 Free PMC article. Review.
References
-
- Howard TJ, Tan T, Lehman GA, et al. Classification and management of perforations complicating endoscopic sphincterotomy. Surgery. 1999;126:658–663. - PubMed
-
- Enns R, Eloubeidi MA, Mergener K, et al. ERCP-related perforations: risk factors and management. Endoscopy. 2002;34:293–298. - PubMed
-
- Assalia A, Suissa A, Ilivitzki A, et al. Validity of clinical criteria in the management of endoscopic retrograde cholangiopancreatography related duodenal perforations. Arch Surg. 2007;142:1059–1064. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
