

Impact of islet size on pancreatic islet transplantation and potential interventions to improve outcome
- PMID: 24143907
- PMCID: PMC4841262
- DOI: 10.3727/096368913X673469
Impact of islet size on pancreatic islet transplantation and potential interventions to improve outcome
Abstract
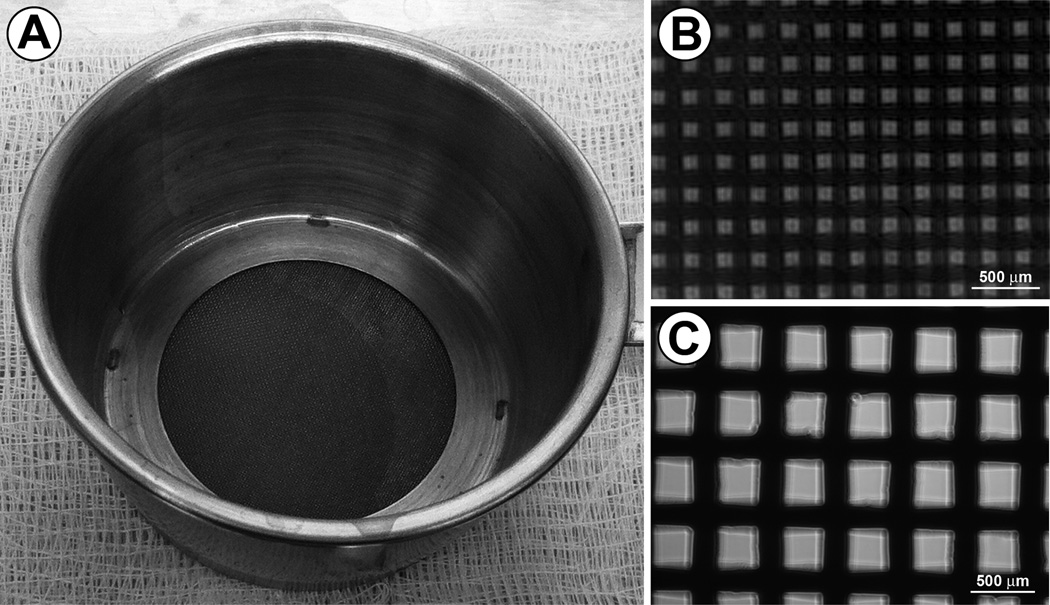
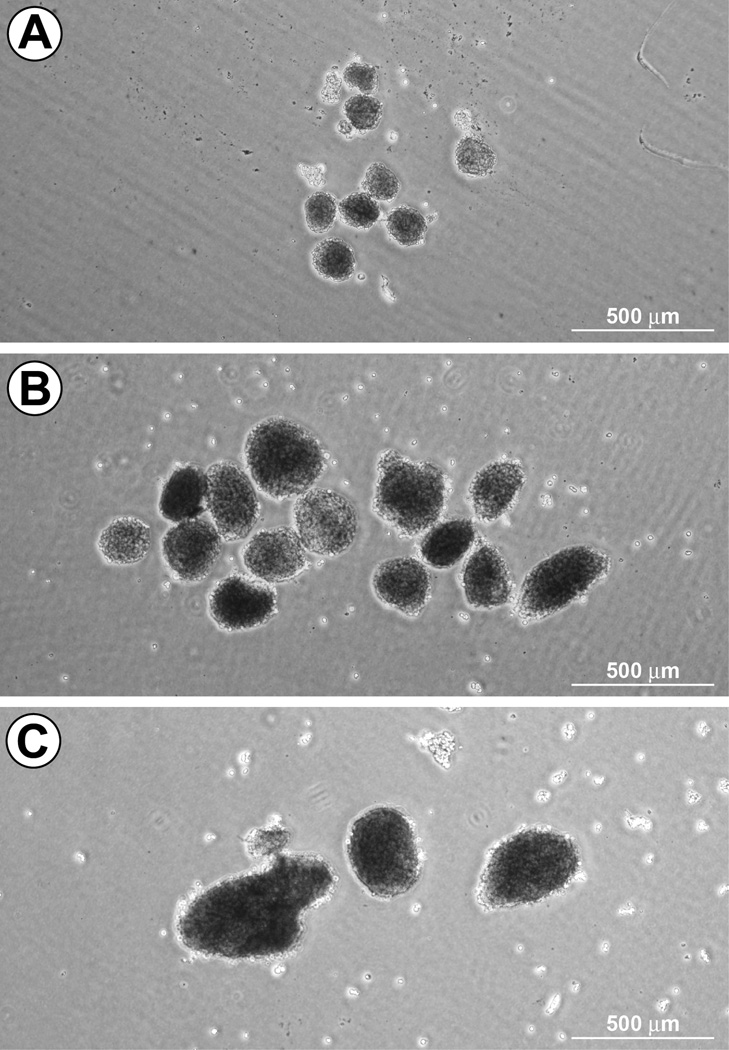
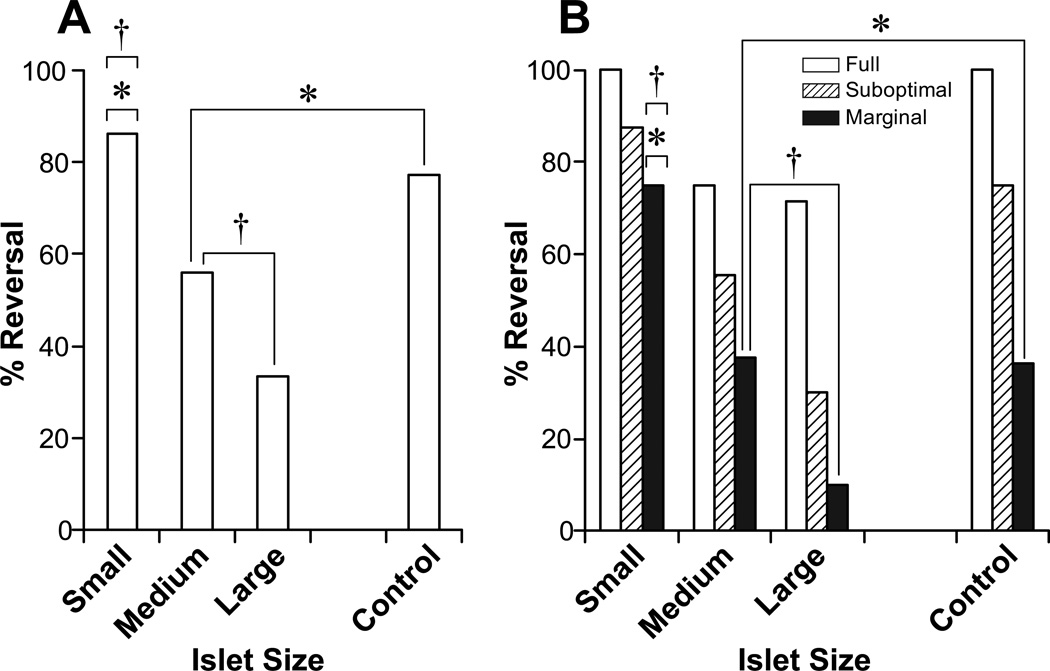
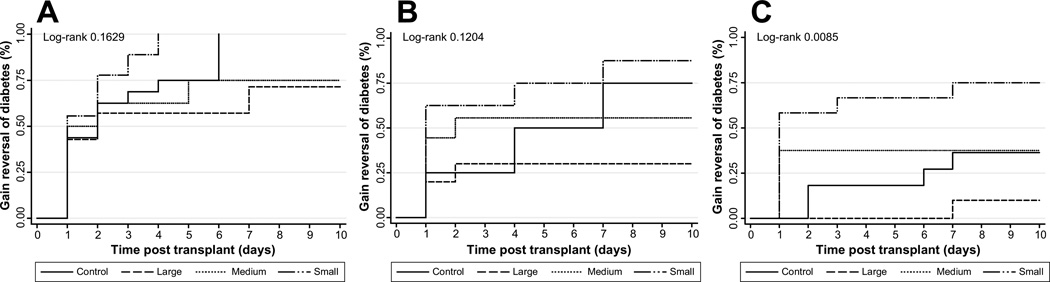
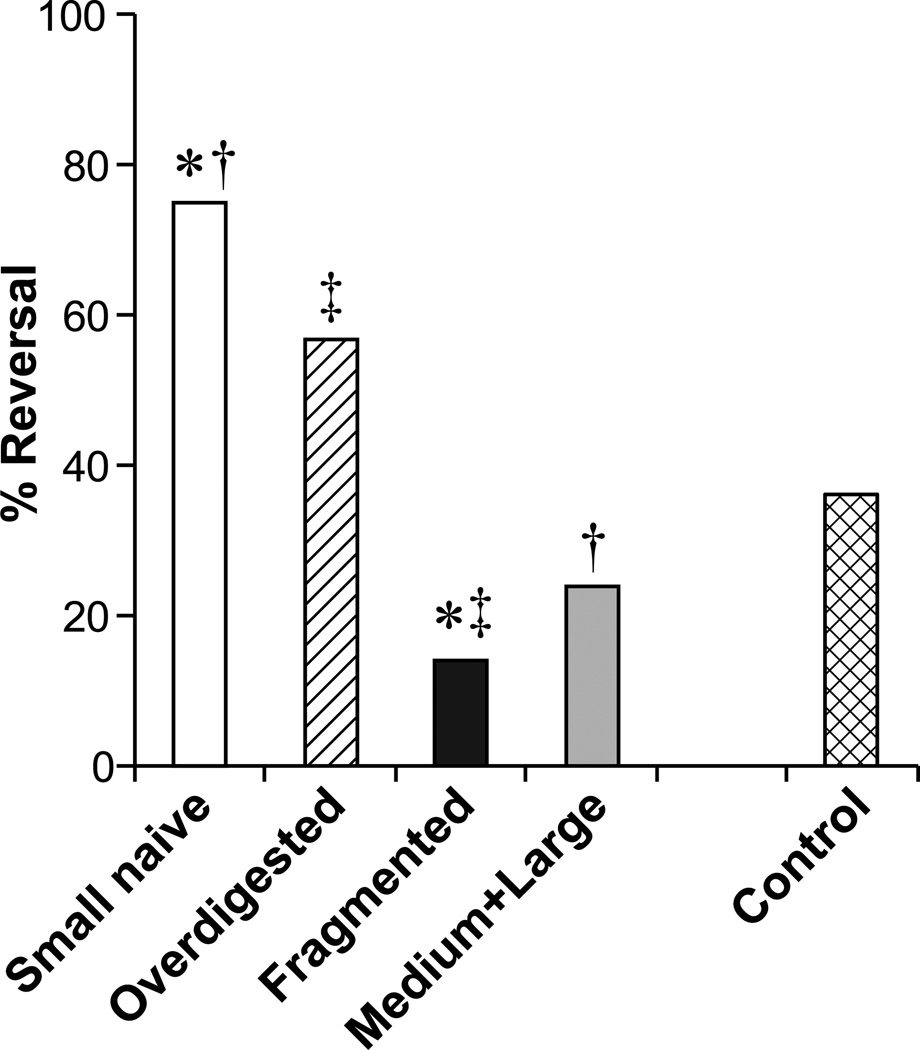
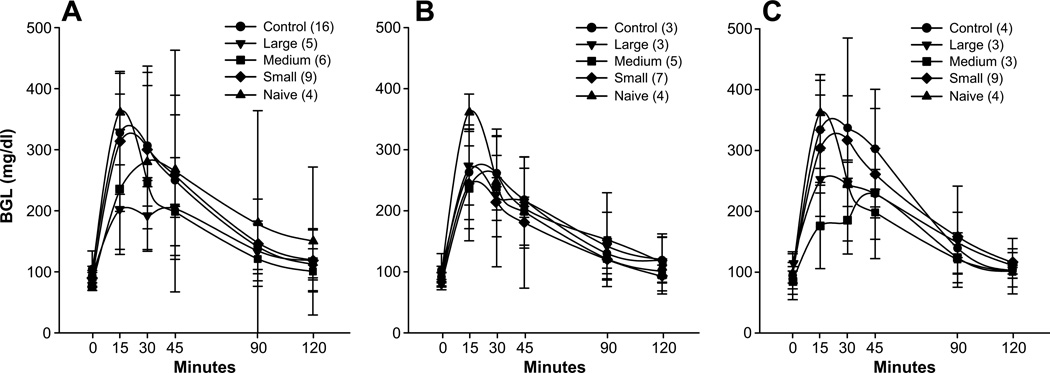
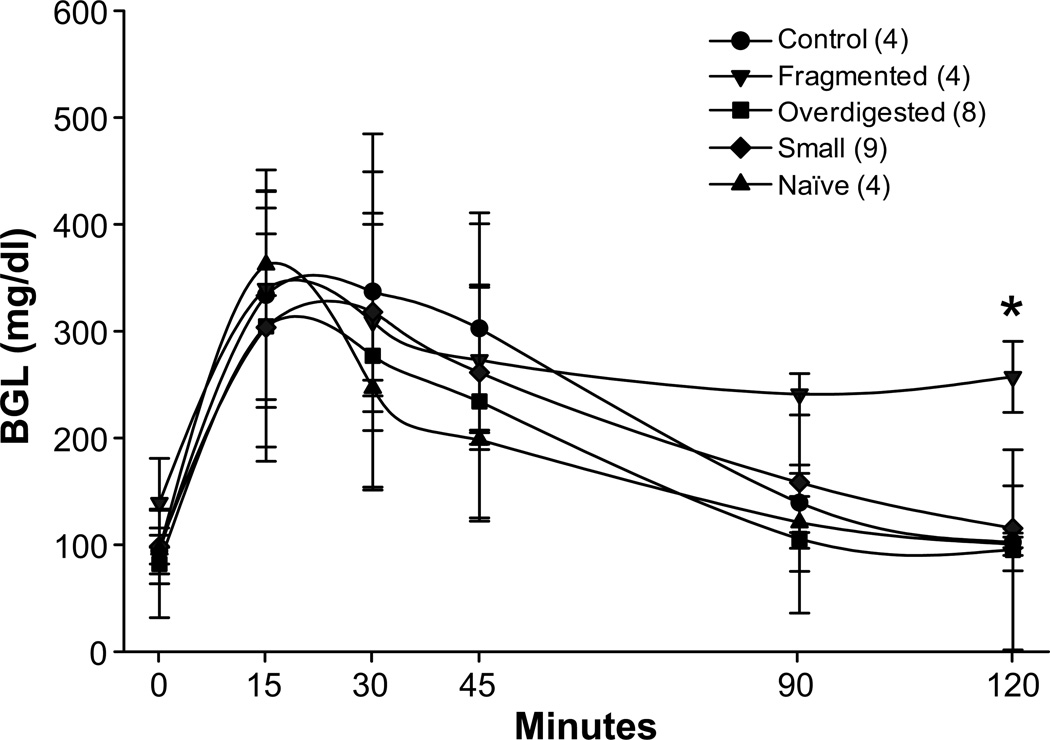
Better results have been recently reported in clinical pancreatic islet transplantation (ITX) due mostly to improved isolation techniques and immunosuppression; however, some limitations still exist. It is known that following transplantation, 30% to 60% of the islets are lost. In our study, we have investigated 1) the role of size as a factor affecting islet engraftment and 2) potential procedural manipulations to increase the number of smaller functional islets that can be transplanted. C57/BL10 mice were used as donors and recipients in a syngeneic islet transplant model. Isolated islets were divided by size (large, >300 μm; medium 150-300 μm; small, <150 μm). Each size was transplanted in chemically induced diabetic mice as full (600 IEQ), suboptimal (400 IEQ), and marginal mass (200 IEQ). Control animals received all size islets. Engraftment was defined as reversal of diabetes by day 7 posttransplantation. When the superiority of smaller islets was observed, strategies of overdigestion and fragmentation were adopted during islet isolation in the attempt to reduce islet size and improve engraftment. Smaller islets were significantly superior in engraftment compared to medium, large, and control (all sizes) groups. This was more evident when marginal mass data were compared. In all masses, success decreased as islet size increased. Once islets were engrafted, functionality was not affected by size. When larger islets were fragmented, a significant decrease in islet functionality was observed. On the contrary, if pancreata were slightly overdigested, although not as successful as small naive islets, an increase in engraftment was observed when compared to the control group. In conclusion, smaller islets are superior in engraftment following islet transplantation. Fragmentation has a deleterious effect on islet engraftment. Islet isolations can be performed by reducing islet size with slight overdigestion, and it can be safely adopted to improve clinical outcome.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Engraftment Site and Effectiveness of the Pan-Caspase Inhibitor F573 to Improve Engraftment in Mouse and Human Islet Transplantation in Mice.Transplantation. 2017 Oct;101(10):2321-2329. doi: 10.1097/TP.0000000000001638. Transplantation. 2017. PMID: 28072753
-
Achievement of insulin independence in three consecutive type-1 diabetic patients via pancreatic islet transplantation using islets isolated at a remote islet isolation center.Transplantation. 2002 Dec 27;74(12):1761-6. doi: 10.1097/00007890-200212270-00020. Transplantation. 2002. PMID: 12499894
-
Factors affecting transplant outcomes in diabetic nude mice receiving human, porcine, and nonhuman primate islets: analysis of 335 transplantations.Transplantation. 2013 Jun 27;95(12):1439-47. doi: 10.1097/TP.0b013e318293b7b8. Transplantation. 2013. PMID: 23677052 Free PMC article.
-
[Experimental and clinical islets transplantation. Current status].Zentralbl Chir. 1992;117(12):670-6. Zentralbl Chir. 1992. PMID: 1285474 Review. German.
-
Therapeutic Strategies for Modulating the Extracellular Matrix to Improve Pancreatic Islet Function and Survival After Transplantation.Curr Diab Rep. 2018 May 19;18(7):39. doi: 10.1007/s11892-018-1014-4. Curr Diab Rep. 2018. PMID: 29779190 Free PMC article. Review.
Cited by
-
Review of Advanced Hydrogel-Based Cell Encapsulation Systems for Insulin Delivery in Type 1 Diabetes Mellitus.Pharmaceutics. 2019 Nov 12;11(11):597. doi: 10.3390/pharmaceutics11110597. Pharmaceutics. 2019. PMID: 31726670 Free PMC article. Review.
-
The Flaws and Future of Islet Volume Measurements.Cell Transplant. 2018 Jul;27(7):1017-1026. doi: 10.1177/0963689718779898. Epub 2018 Jun 28. Cell Transplant. 2018. PMID: 29954219 Free PMC article. Review.
-
Engineering Vascularized Islet Macroencapsulation Devices: An in vitro Platform to Study Oxygen Transport in Perfused Immobilized Pancreatic Beta Cell Cultures.Front Bioeng Biotechnol. 2022 Apr 19;10:884071. doi: 10.3389/fbioe.2022.884071. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 35519615 Free PMC article.
-
Comparison of the Effects of Liraglutide on Islet Graft Survival Between Local and Systemic Delivery.Cell Transplant. 2020 Jan-Dec;29:963689720971245. doi: 10.1177/0963689720971245. Cell Transplant. 2020. PMID: 33172296 Free PMC article.
-
Inhibition of DAI refrains dendritic cells from maturation and prolongs murine islet and skin allograft survival.Front Immunol. 2023 May 1;14:1182851. doi: 10.3389/fimmu.2023.1182851. eCollection 2023. Front Immunol. 2023. PMID: 37197662 Free PMC article.
References
-
- Baca I, Feurle GE, Klempa I, Ziegler A, Schusdziarra V. Morphometry and function of islet cells after different forms of drainage at pancreatic transplantation in rats. Eur. Surg. Res. 1990;22:151–159. - PubMed
-
- Balamurugan AN, Loganathan G, Bellin MD, Wilhelm JJ, Harmon J, Anazawa T, Soltani SM, Radosevich DM, Yuasa T, Tiwari M, Papas KK, McCarthy R, Sutherland DE, Hering BJ. A new enzyme mixture to increase the yield and transplant rate of autologous and allogeneic human islet products. Transplantation. 2012;93:693–702. - PMC - PubMed
-
- Bellin MD, Kandaswamy R, Parkey J, Zhang HJ, Liu B, Ihm SH, Ansite JD, Witson J, Bansal-Pakala P, Balamurugan AN, Papas KK, Sutherland DE, Moran A, Hering BJ. Prolonged insulin independence after islet allotransplants in recipients with type 1 diabetes. Am. J. Transplant. 2008;8:2463–2470. - PMC - PubMed
-
- Bertuzzi F, Ricordi C. Prediction of clinical outcome in islet allotransplantation. Diabetes Care. 2007;30:410–417. - PubMed
-
- Blondet JJ, Carlson AM, Kobayashi T, Jie T, Bellin M, Hering BJ, Freeman ML, Beilman GJ, Sutherland DE. The role of total pancreatectomy and islet autotransplantation for chronic pancreatitis. Surg. Clin. North Am. 2007;87:1477–1501. x. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
