

Risk factors for intra-abdominal hypertension and abdominal compartment syndrome among adult intensive care unit patients: a systematic review and meta-analysis
- PMID: 24144138
- PMCID: PMC4057241
- DOI: 10.1186/cc13075
Risk factors for intra-abdominal hypertension and abdominal compartment syndrome among adult intensive care unit patients: a systematic review and meta-analysis
Abstract
Introduction: Although intra-abdominal hypertension (IAH) and abdominal compartment syndrome (ACS) are associated with substantial morbidity and mortality among critically ill adults, it remains unknown if prevention or treatment of these conditions improves patient outcomes. We sought to identify evidence-based risk factors for IAH and ACS in order to guide identification of the source population for future IAH/ACS treatment trials and to stratify patients into risk groups based on prognosis.
Methods: We searched electronic bibliographic databases (MEDLINE, EMBASE, PubMed, and the Cochrane Database from 1950 until January 21, 2013) and reference lists of included articles for observational studies reporting risk factors for IAH or ACS among adult ICU patients. Identified risk factors were summarized using formal narrative synthesis techniques alongside a random effects meta-analysis.
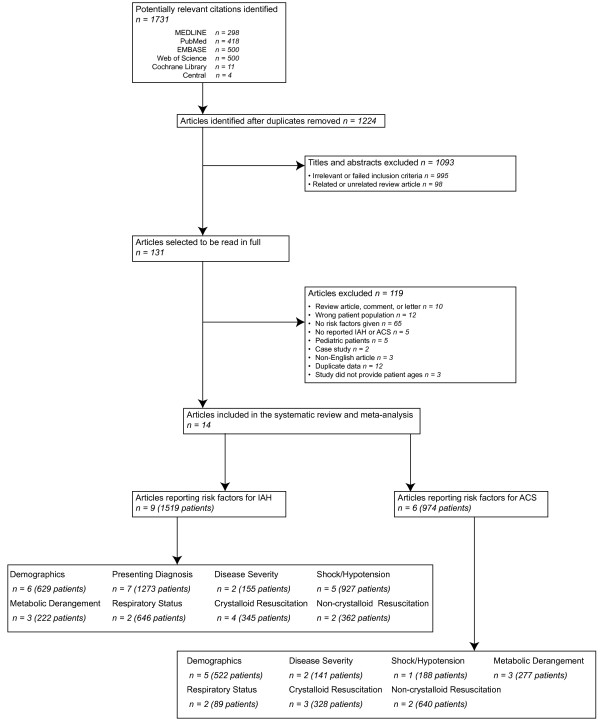
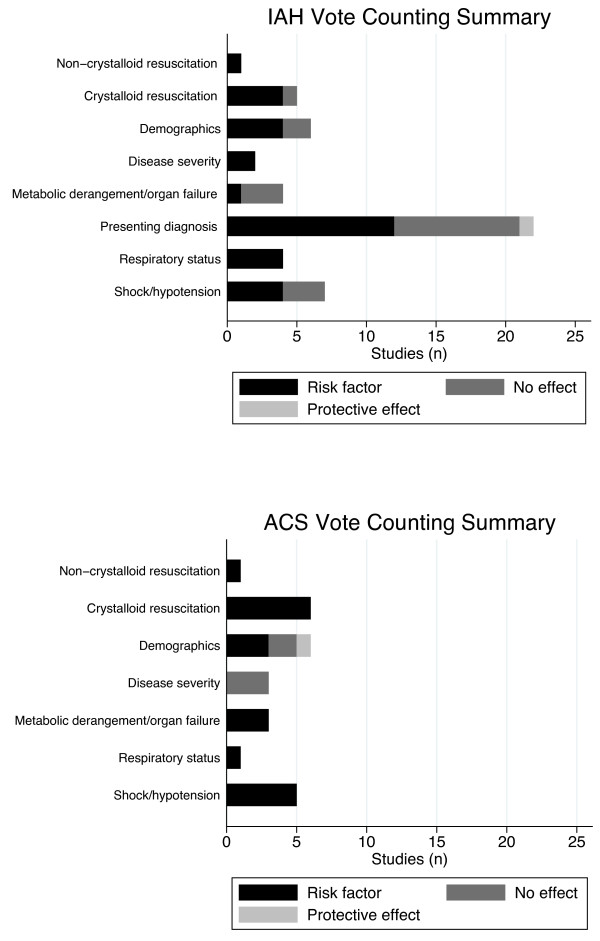
Results: Among 1,224 citations identified, 14 studies enrolling 2,500 patients were included. The 38 identified risk factors for IAH and 24 for ACS could be clustered into three themes and eight subthemes. Large volume crystalloid resuscitation, the respiratory status of the patient, and shock/hypotension were common risk factors for IAH and ACS that transcended across presenting patient populations. Risk factors with pooled evidence supporting an increased risk for IAH among mixed ICU patients included obesity (four studies; odds ratio (OR) 5.10; 95% confidence interval (CI), 1.92 to 13.58), sepsis (two studies; OR 2.38; 95% CI, 1.34 to 4.23), abdominal surgery (four studies; OR 1.93; 95% CI, 1.30 to 2.85), ileus (two studies; OR 2.05; 95% CI, 1.40 to 2.98), and large volume fluid resuscitation (two studies; OR 2.17; 95% CI, 1.30 to 3.63). Among trauma and surgical patients, large volume crystalloid resuscitation and markers of shock/hypotension and metabolic derangement/organ failure were risk factors for IAH and ACS while increased disease severity scores and elevated creatinine were risk factors for ACS in severe acute pancreatitis patients.
Conclusions: Although several IAH/ACS risk factors transcend across presenting patient diagnoses, some appear specific to the population under study. As our findings were somewhat limited by included study methodology, the risk factors reported in this study should be considered candidate risk factors until confirmed by a large prospective multi-centre observational study.
Figures
References
-
- Malbrain MLNG, Chiumello D, Pelosi P, Wilmer A, Brienza N, Malcangi V, Bihari D, Innes R, Cohen J, Singer P, Japiassu A, Kurtop E, De Keulenaer BL, Daelemans R, Del Turco M, Cosimini P, Ranieri M, Jacquet L, Laterre PF, Gattinoni L. Prevalence of intra-abdominal hypertension in critically ill patients: a multi centre epidemiological study. Intensive Care Med. 2004;17:822–829. doi: 10.1007/s00134-004-2169-9. - DOI - PubMed
-
- McBeth PB, Leger C, Ball CG, Ouelett J-F, Laupland KB, Kubes P, Roberts DJ, Shahpori R, Kirkpatrick AW. Intra-abdominal hypertension and intra-abdominal sepsis: critical concepts and possibilities. Int J Intensive Care. 2011;17:10–19.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
