

Concordance of effects of medical interventions on hospital admission and readmission rates with effects on mortality
- PMID: 24144601
- PMCID: PMC3855143
- DOI: 10.1503/cmaj.130430
Concordance of effects of medical interventions on hospital admission and readmission rates with effects on mortality
Abstract
Background: Many clinical trials examine a composite outcome of admission to hospital and death, or infer a relationship between hospital admission and survival benefit. This assumes concordance of the outcomes "hospital admission" and "death." However, whether the effects of a treatment on hospital admissions and readmissions correlate to its effect on serious outcomes such as death is unknown. We aimed to assess the correlation and concordance of effects of medical interventions on admission rates and mortality.
Methods: We searched the Cochrane Database of Systematic Reviews from its inception to January 2012 (issue 1, 2012) for systematic reviews of treatment comparisons that included meta-analyses for both admission and mortality outcomes. For each meta-analysis, we synthesized treatment effects on admissions and death, from respective randomized trials reporting those outcomes, using random-effects models. We then measured the concordance of directions of effect sizes and the correlation of summary estimates for the 2 outcomes.
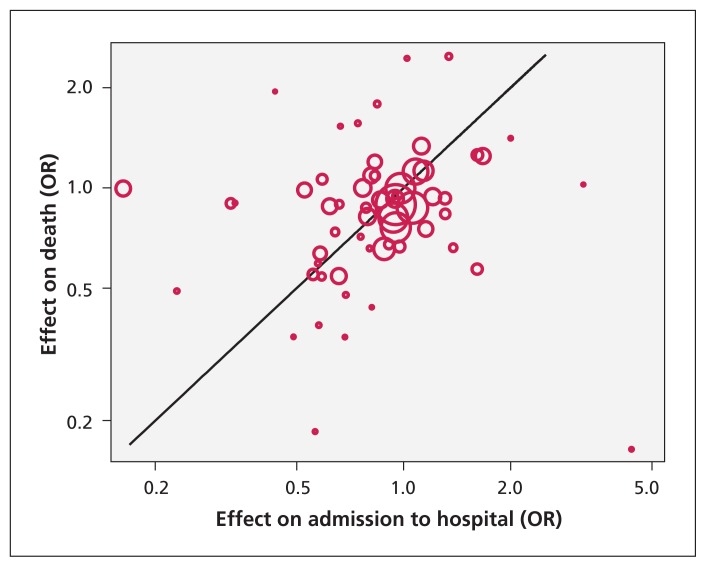
Results: We identified 61 meta-analyses including 398 trials reporting mortality and 182 trials reporting admission rates; 125 trials reported both outcomes. In 27.9% of comparisons, the point estimates of treatment effects for the 2 outcomes were in opposite directions; in 8.2% of trials, the 95% confidence intervals did not overlap. We found no significant correlation between effect sizes for admission and death (Pearson r = 0.07, p = 0.6). Our results were similar when we limited our analysis to trials reporting both outcomes.
Interpretation: In this metaepidemiological study, admission and mortality outcomes did not correlate, and discordances occurred in about one-third of the treatment comparisons included in our analyses. Both outcomes convey useful information and should be reported separately, but extrapolating the benefits of admission to survival is unreliable and should be avoided.
Figures


References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009;360:1418–28 - PubMed
-
- Joynt KE, Jha AK. Thirty-day readmissions — truth and consequences. N Engl J Med 2012;366:1366–9 - PubMed
-
- Freemantle N, Calvert M, Wood J, et al. Composite outcomes in randomized trials: Greater precision but with greater uncertainty? JAMA 2003;289:2554–9 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources