

Alpha-1-adrenergic receptors in heart failure: the adaptive arm of the cardiac response to chronic catecholamine stimulation
- PMID: 24145181
- PMCID: PMC3980029
- DOI: 10.1097/FJC.0000000000000032
Alpha-1-adrenergic receptors in heart failure: the adaptive arm of the cardiac response to chronic catecholamine stimulation
Abstract
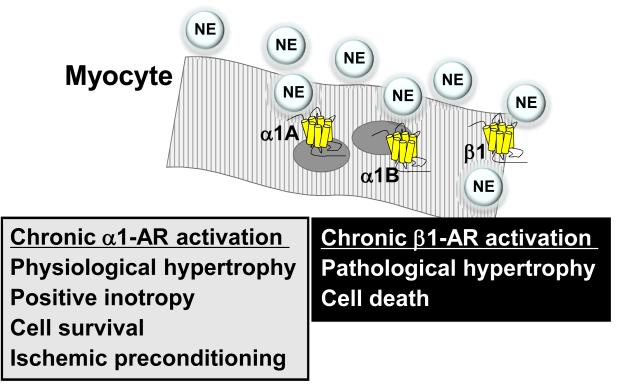
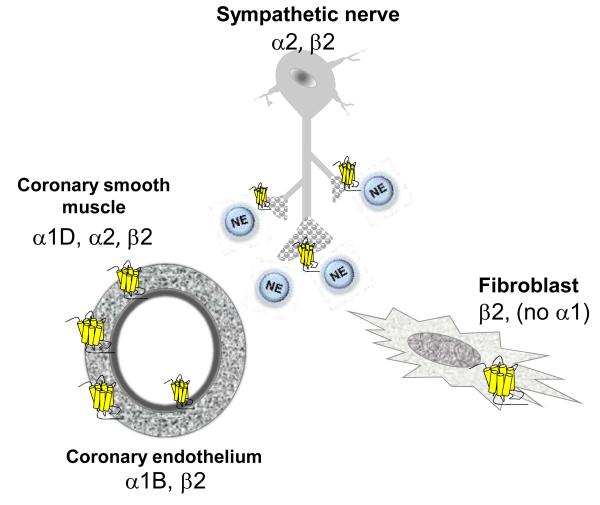
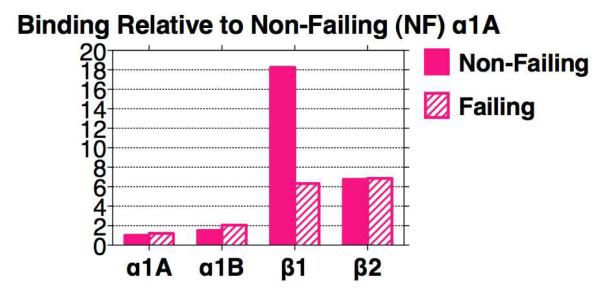
Alpha-1-adrenergic receptors (ARs) are G protein-coupled receptors activated by catecholamines. The alpha-1A and alpha-1B subtypes are expressed in mouse and human myocardium, whereas the alpha-1D protein is found only in coronary arteries. There are far fewer alpha-1-ARs than beta-ARs in the nonfailing heart, but their abundance is maintained or increased in the setting of heart failure, which is characterized by pronounced chronic elevation of catecholamines and beta-AR dysfunction. Decades of evidence from gain and loss-of-function studies in isolated cardiac myocytes and numerous animal models demonstrate important adaptive functions for cardiac alpha-1-ARs to include physiological hypertrophy, positive inotropy, ischemic preconditioning, and protection from cell death. Clinical trial data indicate that blocking alpha-1-ARs is associated with incident heart failure in patients with hypertension. Collectively, these findings suggest that alpha-1-AR activation might mitigate the well-recognized toxic effects of beta-ARs in the hyperadrenergic setting of chronic heart failure. Thus, exogenous cardioselective activation of alpha-1-ARs might represent a novel and viable approach to the treatment of heart failure.
Figures
Similar articles
-
Cardiac α1A-adrenergic receptors: emerging protective roles in cardiovascular diseases.Am J Physiol Heart Circ Physiol. 2021 Feb 1;320(2):H725-H733. doi: 10.1152/ajpheart.00621.2020. Epub 2020 Dec 4. Am J Physiol Heart Circ Physiol. 2021. PMID: 33275531 Free PMC article. Review.
-
Heart failure switches the RV alpha1-adrenergic inotropic response from negative to positive.Am J Physiol Heart Circ Physiol. 2010 Mar;298(3):H913-20. doi: 10.1152/ajpheart.00259.2009. Epub 2009 Dec 24. Am J Physiol Heart Circ Physiol. 2010. PMID: 20035030 Free PMC article.
-
The alpha(1A/C)- and alpha(1B)-adrenergic receptors are required for physiological cardiac hypertrophy in the double-knockout mouse.J Clin Invest. 2003 Jun;111(11):1783-91. doi: 10.1172/JCI16100. J Clin Invest. 2003. PMID: 12782680 Free PMC article.
-
Both alpha(1A)- and alpha(1B)-adrenergic receptors crosstalk to down regulate beta(1)-ARs in mouse heart: coupling to differential PTX-sensitive pathways.J Mol Cell Cardiol. 2005 Nov;39(5):777-84. doi: 10.1016/j.yjmcc.2005.07.015. Epub 2005 Sep 19. J Mol Cell Cardiol. 2005. PMID: 16171811
-
Effect of alpha1-adrenergic receptors in cardiac pathophysiology.Am Heart J. 2006 Nov;152(5):842-50. doi: 10.1016/j.ahj.2006.05.017. Am Heart J. 2006. PMID: 17070143 Review.
Cited by
-
Dual-omics reveals temporal differences in acute sympathetic stress-induced cardiac inflammation following α1 and β-adrenergic receptors activation.Acta Pharmacol Sin. 2023 Jul;44(7):1350-1365. doi: 10.1038/s41401-022-01048-5. Epub 2023 Feb 3. Acta Pharmacol Sin. 2023. PMID: 36737635 Free PMC article.
-
Antifatigue Effect of Panax Notoginseng Leaves Fermented With Microorganisms: In-vitro and In-vivo Evaluation.Front Nutr. 2022 Feb 22;9:824525. doi: 10.3389/fnut.2022.824525. eCollection 2022. Front Nutr. 2022. PMID: 35273989 Free PMC article.
-
Time and technology will tell: the pathophysiologic basis of neurohormonal modulation in heart failure.Heart Fail Clin. 2014 Oct;10(4):543-57. doi: 10.1016/j.hfc.2014.07.002. Epub 2014 Aug 14. Heart Fail Clin. 2014. PMID: 25217430 Free PMC article. Review.
-
PET Radiotracers for CNS-Adrenergic Receptors: Developments and Perspectives.Molecules. 2020 Sep 3;25(17):4017. doi: 10.3390/molecules25174017. Molecules. 2020. PMID: 32899124 Free PMC article. Review.
-
Impact of Aldosterone on the Failing Myocardium: Insights from Mitochondria and Adrenergic Receptors Signaling and Function.Cells. 2021 Jun 19;10(6):1552. doi: 10.3390/cells10061552. Cells. 2021. PMID: 34205363 Free PMC article. Review.
References
-
- Porter KE, Turner NA. Cardiac fibroblasts: at the heart of myocardial remodeling. Pharmacol Ther. 2009;123(2):255–278. - PubMed
-
- Triposkiadis F, Karayannis G, Giamouzis G, Skoularigis J, Louridas G, Butler J. The sympathetic nervous system in heart failure physiology, pathophysiology, and clinical implications. J Am Coll Cardiol. 2009;54(19):1747–1762. - PubMed
-
- Sakata Y, Hoit BD, Liggett SB, Walsh RA, Dorn GW., 2nd Decompensation of pressure-overload hypertrophy in G alpha q-overexpressing mice. Circulation. 1998;97(15):1488–1495. - PubMed
-
- Ponicke K, Vogelsang M, Heinroth M, et al. Endothelin receptors in the failing and nonfailing human heart. Circulation. 1998;97(8):744–751. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
