

Dose-limiting toxicity after hypofractionated dose-escalated radiotherapy in non-small-cell lung cancer
- PMID: 24145340
- PMCID: PMC3837093
- DOI: 10.1200/JCO.2013.51.5353
Dose-limiting toxicity after hypofractionated dose-escalated radiotherapy in non-small-cell lung cancer
Abstract
Purpose: Local failure rates after radiation therapy (RT) for locally advanced non-small-cell lung cancer (NSCLC) remain high. Consequently, RT dose intensification strategies continue to be explored, including hypofractionation, which allows for RT acceleration that could potentially improve outcomes. The maximum-tolerated dose (MTD) with dose-escalated hypofractionation has not been adequately defined.
Patients and methods: Seventy-nine patients with NSCLC were enrolled on a prospective single-institution phase I trial of dose-escalated hypofractionated RT without concurrent chemotherapy. Escalation of dose per fraction was performed according to patients' stratified risk for radiation pneumonitis with total RT doses ranging from 57 to 85.5 Gy in 25 daily fractions over 5 weeks using intensity-modulated radiotherapy. The MTD was defined as the maximum dose with ≤ 20% risk of severe toxicity.
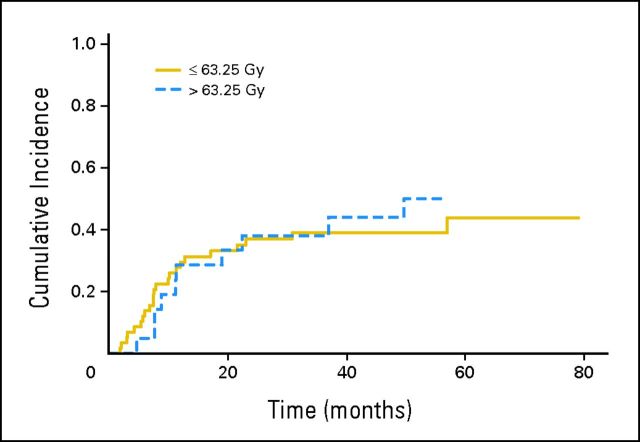
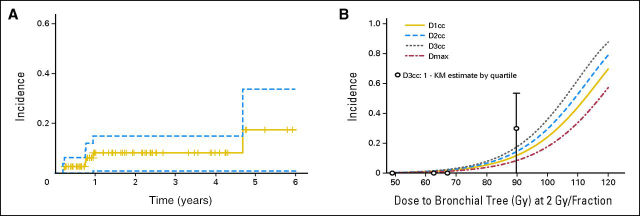
Results: No grade 3 pneumonitis was observed and an MTD for acute toxicity was not identified during patient accrual. However, with a longer follow-up period, grade 4 to 5 toxicity occurred in six patients and was correlated with total dose (P = .004). An MTD was identified at 63.25 Gy in 25 fractions. Late grade 4 to 5 toxicities were attributable to damage to central and perihilar structures and correlated with dose to the proximal bronchial tree.
Conclusion: Although this dose-escalation model limited the rates of clinically significant pneumonitis, dose-limiting toxicity occurred and was dominated by late radiation toxicity involving central and perihilar structures. The identified dose-response for damage to the proximal bronchial tree warrants caution in future dose-intensification protocols, especially when using hypofractionation.
Trial registration: ClinicalTrials.gov NCT00214123.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
[Caution with hypofractionated dose-escalating radiotherapy in non-small cell lung cancer].Strahlenther Onkol. 2014 Jun;190(6):597-9. doi: 10.1007/s00066-014-0667-4. Strahlenther Onkol. 2014. PMID: 24967467 German. No abstract available.
References
-
- Perez CA, Pajak TF, Rubin P, et al. Long-term observations of the patterns of failure in patients with unresectable non-oat cell carcinoma of the lung treated with definitive radiotherapy: Report by the Radiation Therapy Oncology Group. Cancer. 1987;59:1874–1881. - PubMed
-
- Cox JD, Azarnia N, Byhardt RW, et al. A randomized phase I/II trial of hyperfractionated radiation therapy with total doses of 60.0 Gy to 79.2 Gy: Possible survival benefit with greater than or equal to 69.6 Gy in favorable patients with Radiation Therapy Oncology Group stage III non-small-cell lung carcinoma—Report of Radiation Therapy Oncology Group 83-11. J Clin Oncol. 1990;8:1543–1555. - PubMed
-
- Sause W, Kolesar P, Taylor S, IV, et al. Final results of phase III trial in regionally advanced unresectable non-small cell lung cancer: Radiation Therapy Oncology Group, Eastern Cooperative Oncology Group, and Southwest Oncology Group. Chest. 2000;117:358–364. - PubMed
-
- Aupérin A, Le Péchoux C, Rolland E, et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J Clin Oncol. 2010;28:2181–2190. - PubMed
-
- Belderbos JS, Heemsbergen WD, De Jaeger K, et al. Final results of a Phase I/II dose escalation trial in non-small-cell lung cancer using three-dimensional conformal radiotherapy. Int J Radiat Oncol Biol Phys. 2006;66:126–134. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
