

Post-ICU admission fluid balance and pediatric septic shock outcomes: a risk-stratified analysis
- PMID: 24145842
- PMCID: PMC3947064
- DOI: 10.1097/CCM.0b013e3182a64607
Post-ICU admission fluid balance and pediatric septic shock outcomes: a risk-stratified analysis
Abstract
Objective: Observed associations between fluid balance and septic shock outcomes are likely confounded by initial mortality risk. We conducted a risk-stratified analysis of the association between post-ICU admission fluid balance and pediatric septic shock outcomes.
Design: Retrospective analysis of an ongoing multicenter pediatric septic shock clinical and biological database.
Setting: Seventeen PICUs in the United States.
Patients: Three hundred and seventeen children with septic shock.
Interventions: None.
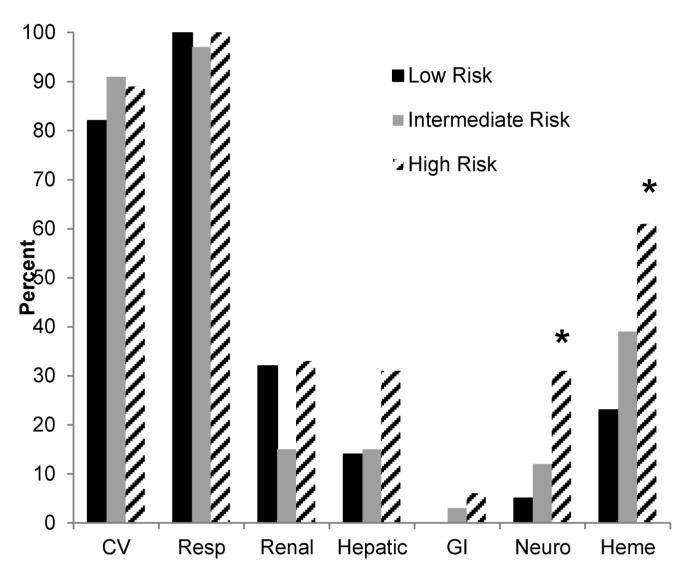
Measurements and main results: We stratified subjects into three mortality risk categories (low, intermediate, and high) using a validated biomarker-based stratification tool. Within each category, we assessed three fluid balance variables: total fluid intake/kg/d during the first 24 hours, percent positive fluid balance during the first 24 hours, and cumulative percent positive fluid balance up to 7 days. We used logistic regression to estimate the effect of fluid balance on the odds of 28-day mortality, and on complicated course, which we defined as either death within 28 days or persistence of two or more organ failures at 7 days. There were 40 deaths, and 91 subjects had a complicated course. Increased cumulative percent positive fluid balance was associated with mortality in the low-risk cohort (n = 204; odds ratio, 1.035; 95% CI, 1.004-1.066) but not in the intermediate- and high-risk cohorts. No other associations with mortality were observed. Fluid intake, percent positive fluid balance in the first 24 hours, and cumulative percent positive fluid balance were all associated with increased odds of a complicated course in the low-risk cohort but not in the intermediate- and high-risk cohorts.
Conclusions: When stratified for mortality risk, increased fluid intake and positive fluid balance after ICU admission are associated with worse outcomes in pediatric septic shock patients with a low initial mortality risk but not in patients at moderate or high mortality risk.
Figures
Comment in
-
Working toward "just right": fluid balance in pediatric septic shock.Crit Care Med. 2014 Feb;42(2):470-1. doi: 10.1097/01.ccm.0000435681.21801.46. Crit Care Med. 2014. PMID: 24434456 No abstract available.
References
-
- Wong HR, Nowak JE, Standage S, de Oliveira CF. In: Sepsis and septic shock. Pediatric critical care medicine. 4th Fuhrman BP, Zimmerman JJ, editors. Mosby; St. Louis: 2011. pp. 1413–1429.
-
- Carcillo JA, Davis AL, Zaritsky A. Role of early fluid resuscitation in pediatric septic shock. JAMA. 1991;266:1242–1245. - PubMed
-
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580–637. - PubMed
-
- de Oliveira CF, de Oliveira DS, Gottschald AF, et al. ACCM/PALS haemodynamic support guidelines for paediatric septic shock: An outcomes comparison with and without monitoring central venous oxygen saturation. Intensive Care Med. 2008;34:1065–1075. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
