

Cornell Assessment of Pediatric Delirium: a valid, rapid, observational tool for screening delirium in the PICU*
- PMID: 24145848
- PMCID: PMC5527829
- DOI: 10.1097/CCM.0b013e3182a66b76
Cornell Assessment of Pediatric Delirium: a valid, rapid, observational tool for screening delirium in the PICU*
Abstract
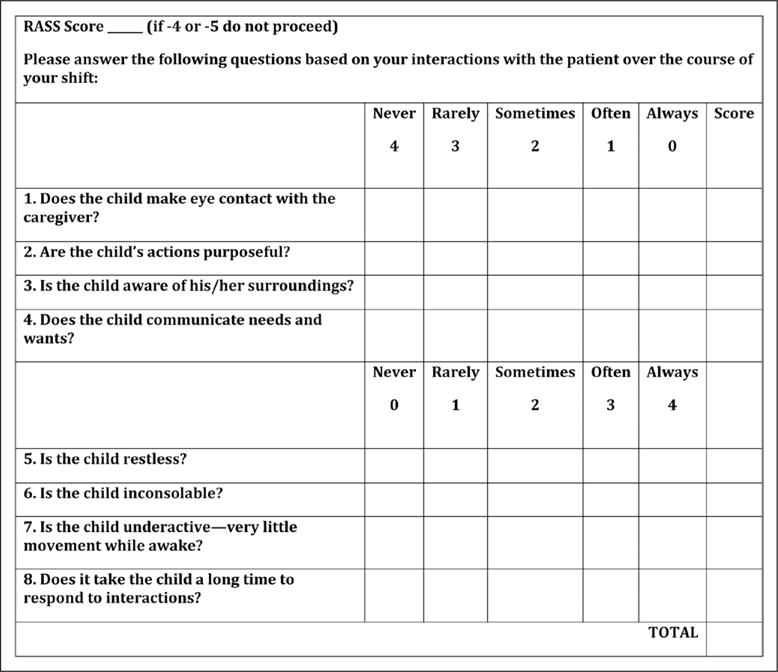
Objective: To determine validity and reliability of the Cornell Assessment of Pediatric Delirium, a rapid observational screening tool.
Design: Double-blinded assessments were performed with the Cornell Assessment of Pediatric Delirium completed by nursing staff in the PICU. These ratings were compared with an assessment by consultation liaison child psychiatrist using the Diagnostic and Statistical Manual IV criteria as the "gold standard" for diagnosis of delirium. An initial series of duplicate Cornell Assessment of Pediatric Delirium assessments were performed in blinded fashion to assess interrater reliability. Nurses recorded the time required to complete the Cornell Assessment of Pediatric Delirium screen.
Setting: Twenty-bed general PICU in a major urban academic medical center over a 10-week period, March-May 2012.
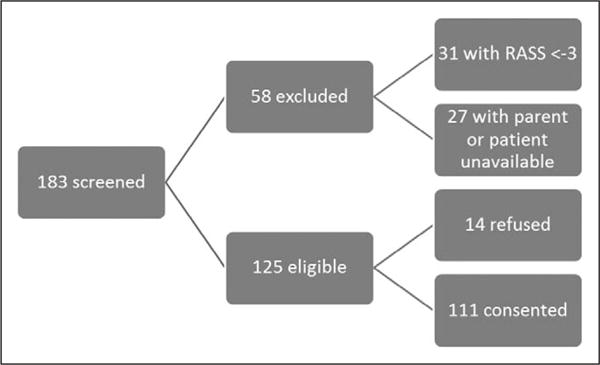
Patients: One hundred eleven patients stratified over ages ranging from 0 to 21 years and across developmental levels.
Intervention: Two hundred forty-eight paired assessments completed.
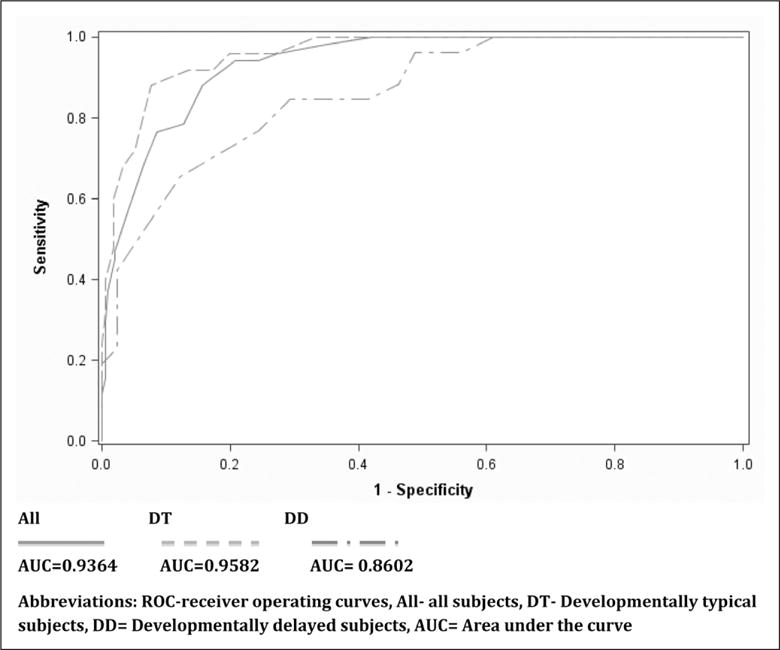
Measurements and main results: The Cornell Assessment of Pediatric Delirium had an overall sensitivity of 94.1% (95% CI, 83.8-98.8%) and specificity of 79.2% (95% CI, 73.5-84.9%). Overall Cronbach's α of 0.90 was observed, with a range of 0.87-0.90 for each of the eight items, indicating good internal consistency. A scoring cut point of 9 demonstrated good interrater reliability of the Cornell Assessment of Pediatric Delirium when comparing results of the screen between nurses (overall κ = 0.94; item range κ = 0.68-0.78). In patients without significant developmental delay, sensitivity was 92.0% (95% CI, 85.7-98.3%) and specificity was 86.5% (95% CI, 75.4-97.6%). In developmentally delayed children, the Cornell Assessment of Pediatric Delirium showed decreased specificity of 51.2% (95% CI, 24.7-77.8%) but sensitivity remained high at 96.2% (95% CI, 86.5-100%). The Cornell Assessment of Pediatric Delirium takes less than 2 minutes to complete.
Conclusions: With an overall prevalence rate of 20.6% in our study population, delirium is a common problem in pediatric critical care. The Cornell Assessment of Pediatric Delirium is a valid, rapid, observational nursing screen that is urgently needed for the detection of delirium in PICU settings.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
On the Cornell Assessment for Pediatric Delirium and both the diagnostic and statistical manual, 5th edition, and International Classification of Diseases, 11th revision: quo vadis?*.Crit Care Med. 2014 Mar;42(3):751-2. doi: 10.1097/01.ccm.0000435686.08339.b6. Crit Care Med. 2014. PMID: 24534972 No abstract available.
-
Rapid diagnosis of PICU delirium.J Pediatr. 2014 Sep;165(3):643. doi: 10.1016/j.jpeds.2014.06.037. J Pediatr. 2014. PMID: 25152157 No abstract available.
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR. Fourth. Washington, DC: American Psychiatric Association; 2000. Task Force on DSM-IV.
-
- Schieveld JN, Leentjens AF. Delirium in severely ill young children in the pediatric intensive care unit (PICU) J Am Acad Child Adolesc Psychiatry. 2005;44:392–394. discussion 395. - PubMed
-
- Martini DR. Commentary: The diagnosis of delirium in pediatric patients. J Am Acad Child Adolesc Psychiatry. 2005;44:395–398. - PubMed
-
- Jakob SM, Ruokonen E, Grounds RM, et al. Dexmedetomidine for Long-Term Sedation Investigators Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: Two randomized controlled trials. JAMA. 2012;307:1151–1160. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
