

Cancer-associated bone disease
- PMID: 24146095
- PMCID: PMC5104551
- DOI: 10.1007/s00198-013-2530-3
Cancer-associated bone disease
Abstract
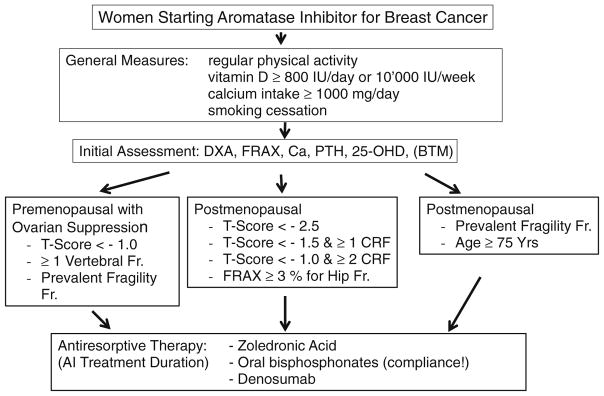
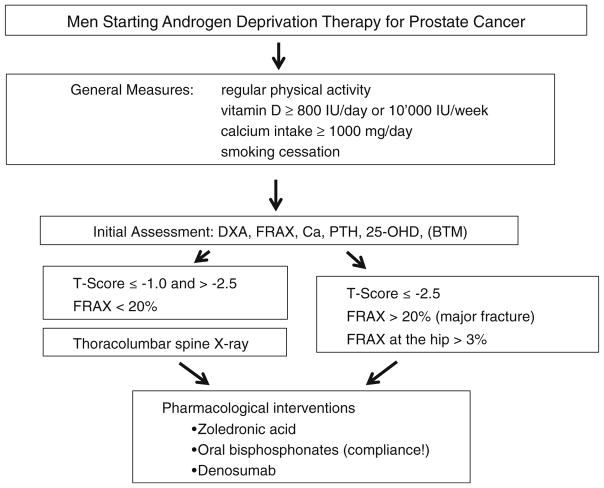
Bone is commonly affected in cancer. Cancer-induced bone disease results from the primary disease, or from therapies against the primary condition, causing bone fragility. Bone-modifying agents, such as bisphosphonates and denosumab, are efficacious in preventing and delaying cancer-related bone disease. With evidence-based care pathways, guidelines assist physicians in clinical decision-making. Of the 57 million deaths in 2008 worldwide, almost two thirds were due to non-communicable diseases, led by cardiovascular diseases and cancers. Bone is a commonly affected organ in cancer, and although the incidence of metastatic bone disease is not well defined, it is estimated that around half of patients who die from cancer in the USA each year have bone involvement. Furthermore, cancer-induced bone disease can result from the primary disease itself, either due to circulating bone resorbing substances or metastatic bone disease, such as commonly occurs with breast, lung and prostate cancer, or from therapies administered to treat the primary condition thus causing bone loss and fractures. Treatment-induced osteoporosis may occur in the setting of glucocorticoid therapy or oestrogen deprivation therapy, chemotherapy-induced ovarian failure and androgen deprivation therapy. Tumour skeletal-related events include pathologic fractures, spinal cord compression, surgery and radiotherapy to bone and may or may not include hypercalcaemia of malignancy while skeletal complication refers to pain and other symptoms. Some evidence demonstrates the efficacy of various interventions including bone-modifying agents, such as bisphosphonates and denosumab, in preventing or delaying cancer-related bone disease. The latter includes treatment of patients with metastatic skeletal lesions in general, adjuvant treatment of breast and prostate cancer in particular, and the prevention of cancer-associated bone disease. This has led to the development of guidelines by several societies and working groups to assist physicians in clinical decision making, providing them with evidence-based care pathways to prevent skeletal-related events and bone loss. The goal of this paper is to put forth an IOF position paper addressing bone diseases and cancer and summarizing the position papers of other organizations.
Conflict of interest statement
René Rizzoli has received speaker or advisory board fees from Amgen, MSD, GSK, Servier, Danone and Takeda. Jean-Jacques Body has received speaker and consulting fees from Amgen and Novartis. Jorge B. Cannata-Andía has received research grants and speaker or advisory board fees from Amgen, Abbott, Servier and Shire. David Kendler has received honoraria for speaking, consulting and/or research grants from Amgen, Novartis, GSK, Eli Lily, Merck, Johnson&Johnson, Pfizer and Roche. Alexandra Papaioannou has been a consultant, or on a speaker’s bureau, or received unrestricted grants from Amgen, Eli Lilly, Merck Canada Inc., Novartis, Pfizer and Warner Chilcott. Tobias J de Villiers has received speaker or advisory board fees from Amgen, Merck, Adcock Ingram and Pfizer. Catherine Van Poznak has received research support from Amgen and Novartis. Ghada El-Hajj Fuleihan has received grants to support courses on osteoporosis from Novartis Pharmaceuticals and Les Laboratoires Servier. Abdellah El Maghraoui, Nicola Napoli, Dominique D Pierroz and Maria Rahme have no conflict of interest.
Figures
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- WHO. Description of the global burden of NCDs, their risk factors and determinants. WHO; Geneva: 2011. Global status report on noncommunicable diseases 2010.
-
- Weigelt B, Peterse JL, van ’t Veer LJ. Breast cancer metastasis: markers and models. Nat Rev Cancer. 2005;5:591–602. - PubMed
-
- Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res. 2006;12:6243s–6249s. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
