

Clinical assessment of anti-viral CD8+ T cell immune monitoring using QuantiFERON-CMV® assay to identify high risk allogeneic hematopoietic stem cell transplant patients with CMV infection complications
- PMID: 24146744
- PMCID: PMC3795724
- DOI: 10.1371/journal.pone.0074744
Clinical assessment of anti-viral CD8+ T cell immune monitoring using QuantiFERON-CMV® assay to identify high risk allogeneic hematopoietic stem cell transplant patients with CMV infection complications
Abstract
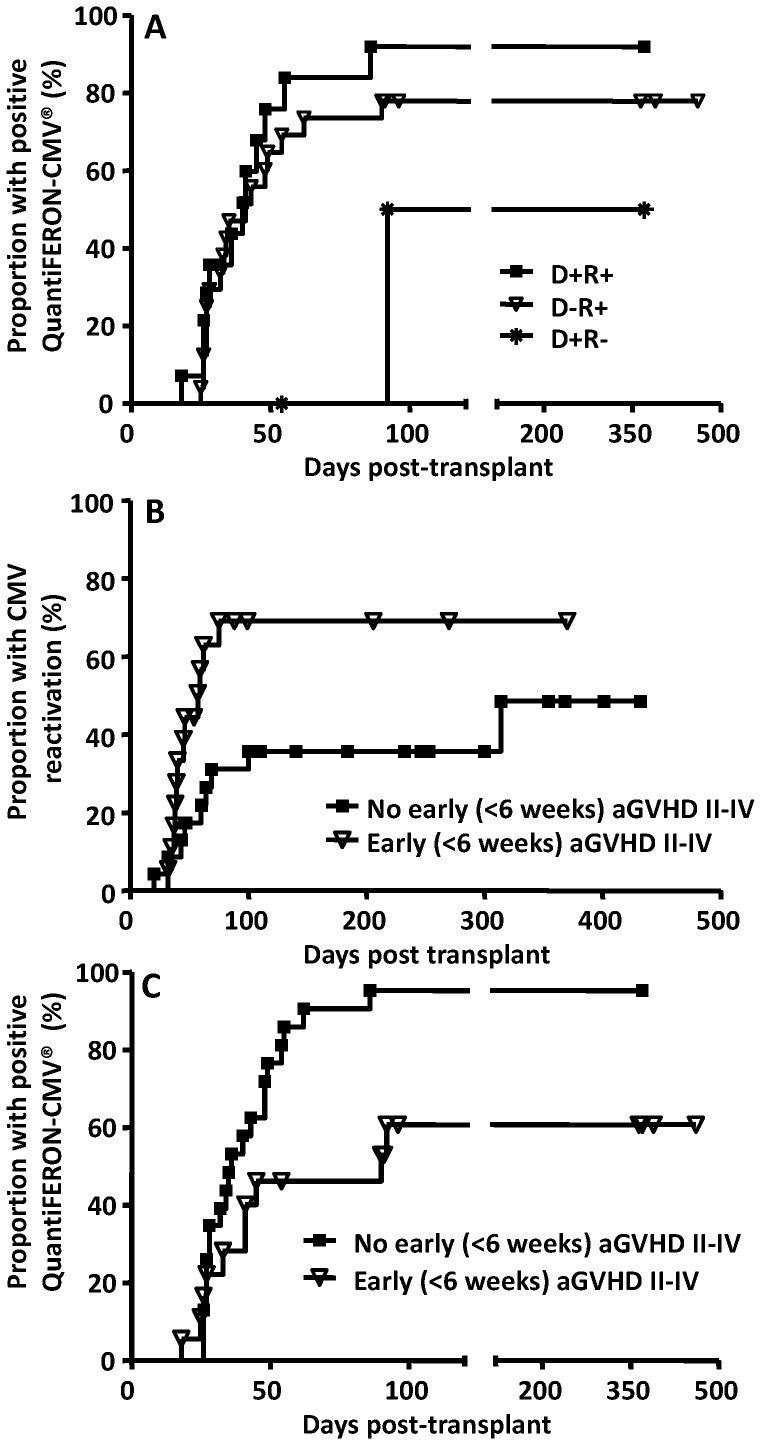
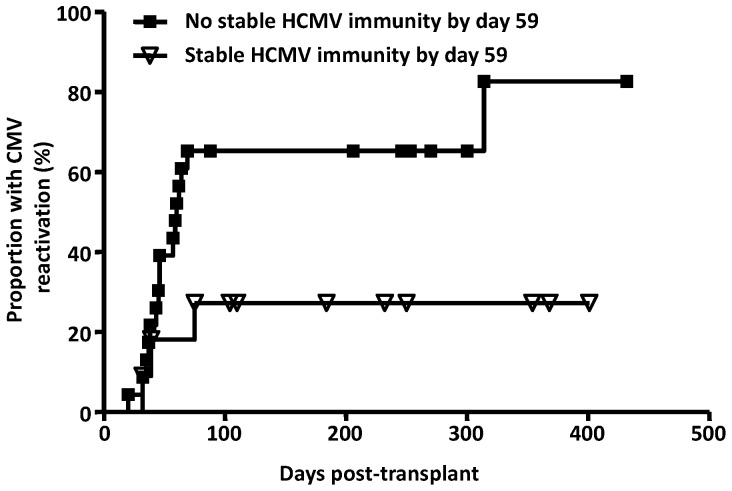
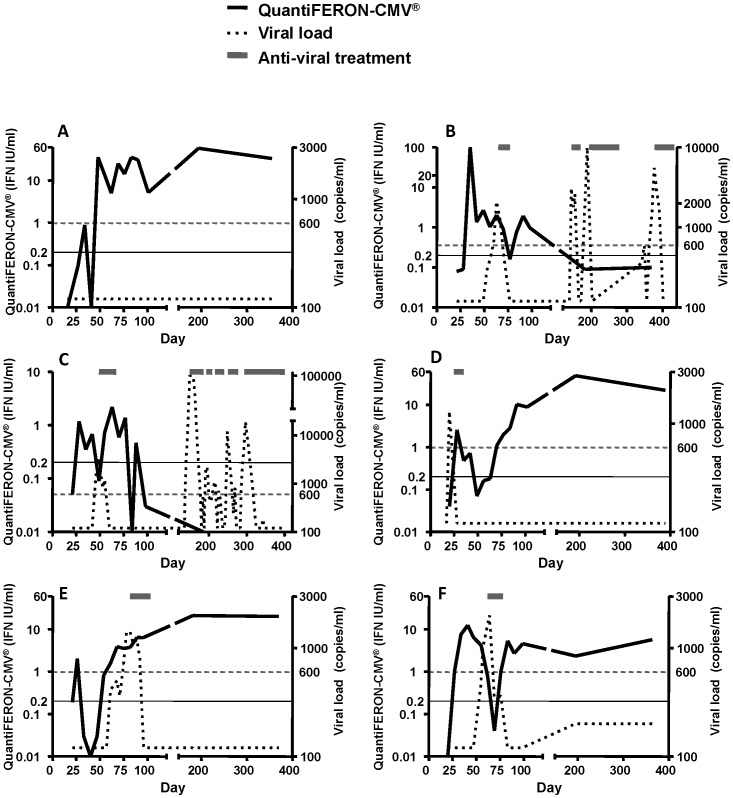
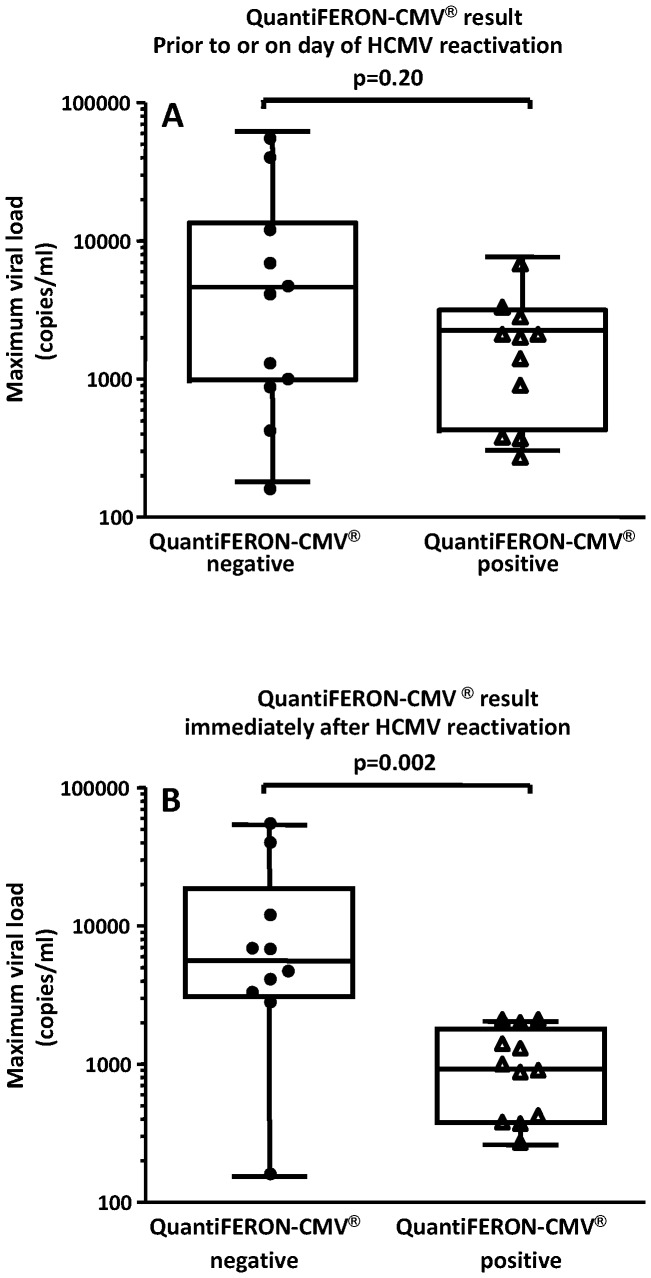
The reconstitution of anti-viral cellular immunity following hematopoietic stem cell transplantation (HSCT) is crucial in preventing cytomegalovirus (CMV)-associated complications. Thus immunological monitoring has emerged as an important tool to better target pre-emptive anti-viral therapies. However, traditional laboratory-based assays are too cumbersome and complicated to implement in a clinical setting. Here we conducted a prospective study of a new whole blood assay (referred to as QuantiFERON-CMV®) to determine the clinical utility of measuring CMV-specific CD8+ T-cell responses as a prognostic tool. Forty-one evaluable allogeneic HSCT recipients underwent weekly immunological monitoring from day 21 post-transplant and of these 21 (51.2%) showed CMV reactivation and 29 (70.7%) developed acute graft-versus-host disease (GvHD). Patients with acute GvHD (grade ≥ 2) within 6 weeks of transplant showed delayed reconstitution of CMV-specific T-cell immunity (p = 0.013) and a higher risk of CMV viremia (p = 0.026). The median time to stable CMV-specific immune reconstitution was 59 days and the incidence of CMV reactivation was lower in patients who developed this than those who did not (27% versus 65%; p = 0.031). Furthermore, a failure to reconstitute CMV-specific immunity soon after the onset of CMV viraemia was associated with higher peak viral loads (5685 copies/ml versus 875 copies/ml; p = 0.002). Hence, QuantiFERON-CMV® testing in the week following CMV viremia can be useful in identifying HSCT recipients at risk of complicated reactivation.
Conflict of interest statement
Figures
References
-
- Gandhi MK, Khanna R (2004) Human cytomegalovirus: clinical aspects, immune regulation, and emerging treatments. Lancet Infect Dis 4: 725–738. - PubMed
-
- Boeckh M, Nichols WG (2004) The impact of cytomegalovirus serostatus of donor and recipient before hematopoietic stem cell transplantation in the era of antiviral prophylaxis and preemptive therapy. Blood 103: 2003–2008. - PubMed
-
- Boeckh M, Nichols WG, Papanicolaou G, Rubin R, Wingard JR, et al. (2003) Cytomegalovirus in hematopoietic stem cell transplant recipients: Current status, known challenges, and future strategies. Biol Blood Marrow Transplant 9: 543–558. - PubMed
-
- Lilleri D, Fornara C, Chiesa A, Caldera D, Alessandrino EP, et al. (2008) Human cytomegalovirus-specific CD4+ and CD8+ T-cell reconstitution in adult allogeneic hematopoietic stem cell transplant recipients and immune control of viral infection. Haematologica 93: 248–256. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
