

How to improve the early diagnosis of Trypanosoma cruzi infection: relationship between validated conventional diagnosis and quantitative DNA amplification in congenitally infected children
- PMID: 24147166
- PMCID: PMC3798617
- DOI: 10.1371/journal.pntd.0002476
How to improve the early diagnosis of Trypanosoma cruzi infection: relationship between validated conventional diagnosis and quantitative DNA amplification in congenitally infected children
Abstract
Background: According to the Chagas congenital transmission guides, the diagnosis of infants, born to Trypanosoma cruzi infected mothers, relies on the detection of parasites by INP micromethod, and/or the persistence of T. cruzi specific antibody titers at 10-12 months of age.
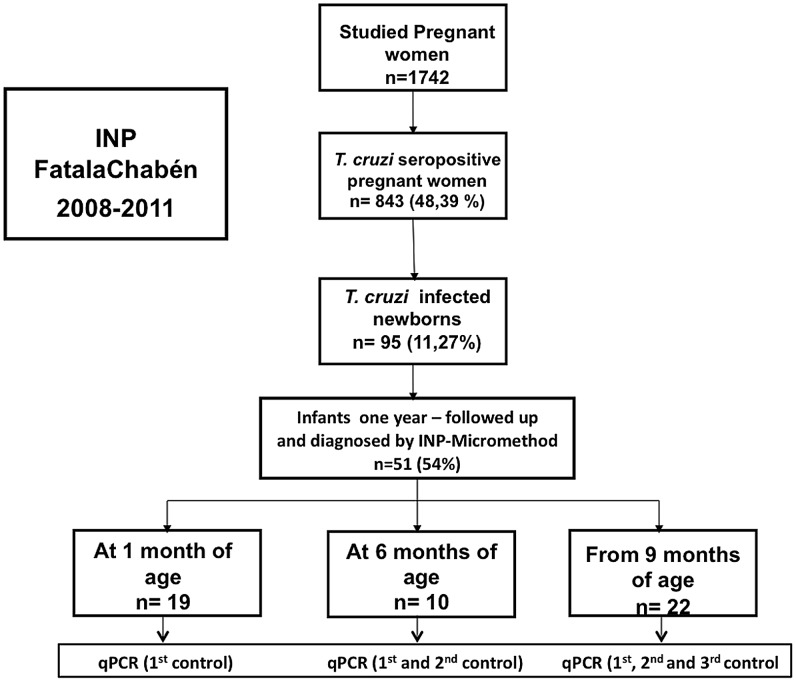
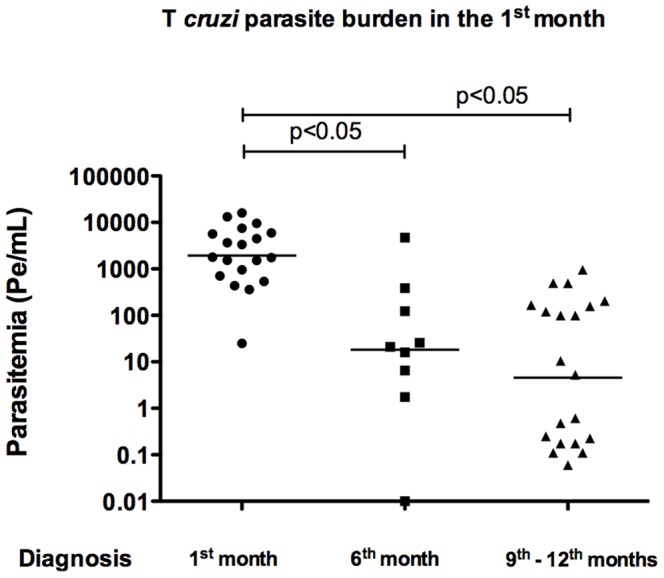
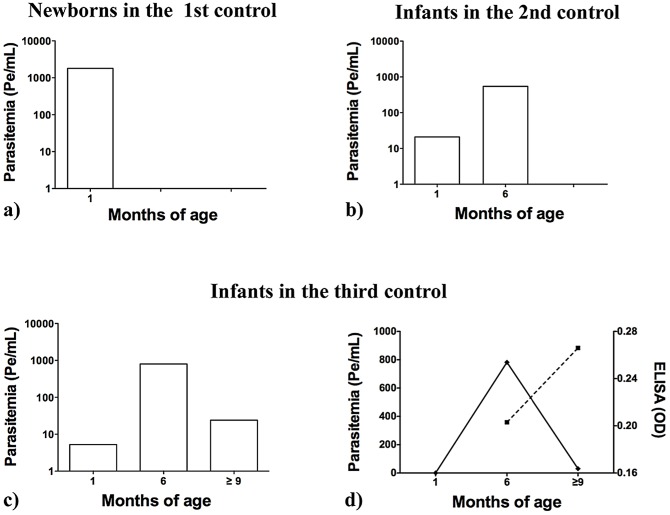
Methodology and principal findings: Parasitemia levels were quantified by PCR in T. cruzi-infected children, grouped according to the results of one-year follow-up diagnosis: A) Neonates that were diagnosed in the first month after delivery by microscopic blood examination (INP micromethod) (n = 19) had a median parasitemia of 1,700 Pe/mL (equivalent amounts of parasite DNA per mL); B) Infants that required a second parasitological diagnosis at six months of age (n = 10) showed a median parasitemia of around 20 Pe/mL and 500 Pe/mL at 1 and 6 months old, respectively, and C) babies with undetectable parasitemia by three blood microscopic observations but diagnosed by specific anti - T. cruzi serology at around 1 year old, (n = 22), exhibited a parasitemia of around 5 Pe/mL, 800 Pe/mL and 20 Pe/mL 1, 6 and 12 month after delivery, respectively. T. cruzi parasites were isolated by hemoculture from 19 congenitally infected children, 18 of which were genotypified as DTU TcV, (former lineage TcIId) and only one as TcI.
Significance: This report is the first to quantify parasitemia levels in more than 50 children congenitally infected with T. cruzi, at three different diagnostic controls during one-year follow-up after delivery. Our results show that the parasite burden in some children (22 out of 51) is below the detection limit of the INP micromethod. As the current trypanocidal treatment proved to be very effective to cure T. cruzi - infected children, more sensitive parasitological methods should be developed to assure an early T. cruzi congenital diagnosis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Rassi A Jr, Rassi A, Marcondes de Rezende J (2012) American trypanosomiasis (Chagas disease). Infect Dis Clin North Am 26: 275–291. - PubMed
-
- Carlier Y, Truyens C, Deloronc F, Peyron F (2012) Congenital parasitic infections: A review. Acta Tropica 121: 55–70. - PubMed
-
- Russomando G, de Tomassone MM, de Guillen I, Acosta N, Vera N, et al. (1998) Treatment of congenital Chagas' disease diagnosed and followed up by the polymerase chain reaction. Am J Trop Med Hyg 59: 487–491. - PubMed
-
- Torrico F, Alonso-Vega C, Suarez E, Rodriguez P, Torrico MC, et al. (2004) Maternal Trypanosoma cruzi infection, pregnancy outcome, morbidity, and mortality of congenitally infected and non-infected newborns in Bolivia. Am J Trop Med Hyg 70: 201–209. - PubMed
-
- Salas NA, Postigo Schneider D, Santalla JA, Brutus L, Chippaux JP (2012) Prevalence of Chagas disease in pregnant women and incidence of congenital transmission in Santa Cruz de la Sierra, Bolivia. Acta Trop 124: 87–91. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
