

Progression from new methicillin-resistant Staphylococcus aureus colonisation to infection: an observational study in a hospital cohort
- PMID: 24148135
- PMCID: PMC4015767
- DOI: 10.1186/1471-2334-13-491
Progression from new methicillin-resistant Staphylococcus aureus colonisation to infection: an observational study in a hospital cohort
Abstract
Background: Patients newly colonised with methicillin-resistant Staphylococcus aureus (MRSA) are at higher risk of clinical MRSA infection. At present, there are limited data on the duration or magnitude of this risk in a hospital population with a known time of MRSA acquisition.
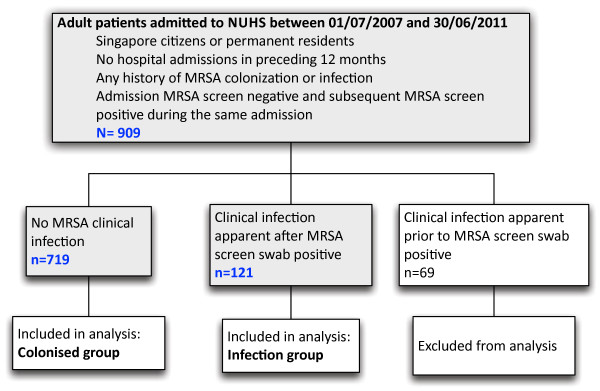
Methods: A retrospective cohort study of 909 adult patients known to have newly identified MRSA colonisation during admission to National University Hospital, Singapore between 1 July 2007 and 30 June 2011 was undertaken. Patients were excluded if they had history of previous MRSA colonisation or infection, or if they had been a hospital inpatient in the preceding 12 months. Data were collected on the development of MRSA infection requiring hospitalisation up to 30 June 2012.
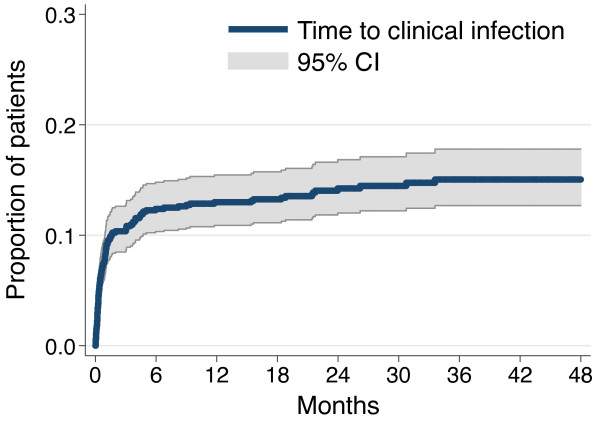
Results: Of 840 patients newly colonised with MRSA as identified on active surveillance and not clinical specimens, 546 were men (65.0%) and the median age was 65 years (range 18-103 years). Median follow up was 24 months (range 0 -64 months, 85.1% followed >6 months). Clinical infection occurred in 121 patients (14.4%) with median time to infection of 22 days (95% CI 14-31). Overall 71.9% (87/121) of infected patients developed infection within 60 days of the date MRSA colonisation was detected. However, 17/121 patients (14.0%) developed clinical infection more than six months after documented MRSA acquisition. The most common sites of clinical infection were skin and soft tissue (49/121, 40.5%, 95% CI 31.7-49.8), respiratory tract (37/121, 30.6%, 95% CI 22.5-39.6) and bone and joint infections (14/121, 11.6%, 95% CI 6.5-18.7). Thirteen patients (13/121, 10.7%, 95% CI 5.8-17.7) had bacteraemias, of which six (5.0% 95% CI 1.8-10.5) were primary and seven (5.7%, 95% CI 2.3-11.6) were secondary to infection at other sites. Crude mortality at 30 days and six months was higher in patients with MRSA infection than colonisation alone (aOR 5.49, 95% CI 2.75-10.95, p<0.001 and aOR 2.94, 95% CI 1.78-4.85, p<0.001 respectively).
Conclusion: Risk of clinical infection is highest soon after MRSA acquisition. Prevention of MRSA acquisition in hospital will have significant impact on morbidity and mortality for patients.
Figures
References
-
- Sievert DM, Ricks P, Edwards JR, Schneider A, Patel J, Srinivasan A, Kallen A, Limbago B, Fridkin S. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect Control Hosp Epidemiol. 2013;13:1–14. - PubMed
-
- Cosgrove SE, Qi Y, Kaye KS, Harbarth S, Karchmer AW, Carmeli Y. The impact of methicillin resistance in Staphylococcus aureus bacteremia on patient outcomes: mortality, length of stay, and hospital charges. Infect Control Hosp Epidemiol. 2005;13:166–174. - PubMed
-
- Shorr AF. Epidemiology and economic impact of meticillin-resistant Staphylococcus aureus: review and analysis of the literature. Pharmacoeconomics. 2007;13:751–768. - PubMed
-
- Pada SK, Ding Y, Ling ML, Hsu LY, Earnest A, Lee TE, Yong HC, Jureen R, Fisher D. Economic and clinical impact of nosocomial meticillin-resistant Staphylococcus aureus infections in Singapore: a matched case–control study. J Hosp Infect. 2011;13:36–40. - PubMed
-
- Huang SS, Diekema DJ, Warren DK, Zuccotti G, Winokur PL, Tendolkar S, Boyken L, Datta R, Jones RM, Ward MA, Aubrey T, Onderdonk AB, Garcia C, Platt R. Strain-relatedness of methicillin-resistant Staphylococcus aureus isolates recovered from patients with repeated infection. Clin Infect Dis. 2008;13:1241–1247. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
