

Providing clinicians with a patient's 10-year cardiovascular risk improves their statin prescribing: a true experiment using clinical vignettes
- PMID: 24148829
- PMCID: PMC3924357
- DOI: 10.1186/1471-2261-13-90
Providing clinicians with a patient's 10-year cardiovascular risk improves their statin prescribing: a true experiment using clinical vignettes
Abstract
Background: Statins are effective for primary prevention of cardiovascular (CV) disease, the leading cause of death in the world. Multinational guidelines emphasize CV risk as an important factor for optimal statin prescribing. However, it's not clear how primary care providers (PCPs) use this information. The objective of this study was to determine how primary care providers use information about global CV risk for primary prevention of CV disease.
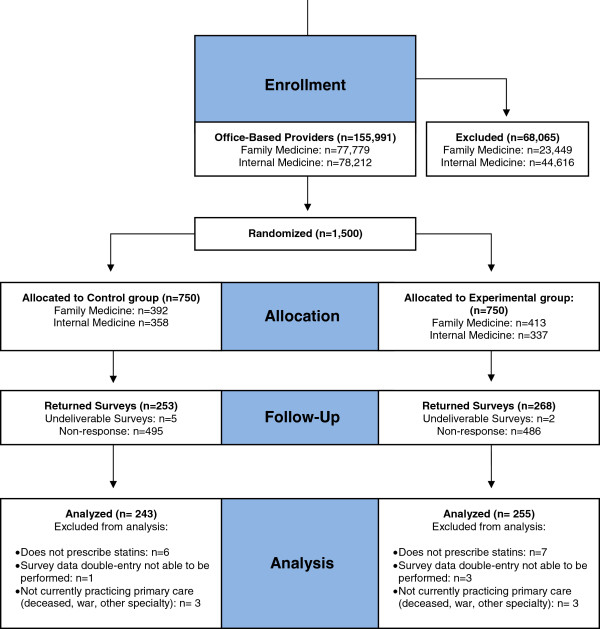
Methods: A double-blinded, randomized experiment using clinical vignettes mailed to office-based PCPs in the United States who were identified through the American Medical Association Physician Masterfile in June 2012. PCPs in the control group received clinical vignettes with all information on the risk factors needed to calculate CV risk. The experimental group received the same vignettes in addition to the subject's 10-year calculated CV risk (Framingham risk score). The primary study outcome was the decision to prescribe a statin.
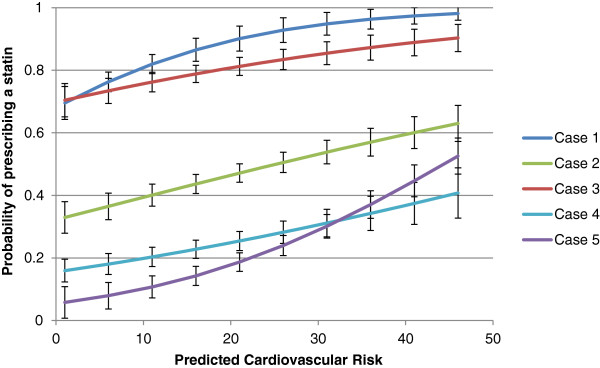
Results: Providing calculated CV risk to providers increased statin prescribing in the two high-risk cases (CV risk > 20%) by 32 percentage points (41% v. 73%; 95% CI = 23-40, p <0.001; relative risk [RR] = 1.78) and 16 percentage points (12% v. 27%, 95% CI 8.5-22.5%, p <0.001; RR = 2.25), and decreased statin prescribing in the lowest risk case (CV risk = 2% risk) by 9 percentage points [95% CI = 1.00-16.7%, p = 0.003, RR = 0.88]. Fewer than 20% of participants in each group reported routinely calculating 10-year CV risk in their patients.
Conclusions: Providers do not routinely calculate 10-year CV risk for their patients. In this vignette experiment, PCPs undertreated low LDL, high CV risk patients. Giving providers a patient's calculated CV risk improved statin prescribing. Providing PCPs with accurate estimates of patient CV risk at the point of service has the potential to improve the efficiency of statin prescribing.
Figures
Similar articles
-
Effect of an Automated Patient Dashboard Using Active Choice and Peer Comparison Performance Feedback to Physicians on Statin Prescribing: The PRESCRIBE Cluster Randomized Clinical Trial.JAMA Netw Open. 2018 Jul 6;1(3):e180818. doi: 10.1001/jamanetworkopen.2018.0818. JAMA Netw Open. 2018. PMID: 30646039 Free PMC article. Clinical Trial.
-
Statin prescribing in the elderly in the Netherlands: a pharmacy database time trend study.Drugs Aging. 2010 Jul 1;27(7):589-96. doi: 10.2165/11537330-000000000-00000. Drugs Aging. 2010. PMID: 20583852
-
Association of Primary Care Providers' Beliefs of Statins for Primary Prevention and Statin Prescription.J Am Heart Assoc. 2019 Feb 5;8(3):e010241. doi: 10.1161/JAHA.118.010241. J Am Heart Assoc. 2019. PMID: 30681391 Free PMC article.
-
Effectiveness of Interventions Aimed at Increasing Statin-Prescribing Rates in Primary Cardiovascular Disease Prevention: A Systematic Review of Randomized Clinical Trials.JAMA Cardiol. 2019 Nov 1;4(11):1160-1169. doi: 10.1001/jamacardio.2019.3066. JAMA Cardiol. 2019. PMID: 31461127
-
Evidence-based prescribing: combining network meta-analysis with multicriteria decision analysis to choose among multiple drugs.Circ Cardiovasc Qual Outcomes. 2014 Sep;7(5):787-92. doi: 10.1161/CIRCOUTCOMES.114.000825. Epub 2014 Aug 5. Circ Cardiovasc Qual Outcomes. 2014. PMID: 25097214 Review. No abstract available.
Cited by
-
Quality Improvement and Personalization for Statins: the QUIPS Quality Improvement Randomized Trial of Veterans' Primary Care Statin Use.J Gen Intern Med. 2018 Dec;33(12):2132-2137. doi: 10.1007/s11606-018-4681-6. Epub 2018 Oct 3. J Gen Intern Med. 2018. PMID: 30284172 Free PMC article. Clinical Trial.
-
Use of electronic health record data and machine learning to identify candidates for HIV pre-exposure prophylaxis: a modelling study.Lancet HIV. 2019 Oct;6(10):e688-e695. doi: 10.1016/S2352-3018(19)30137-7. Epub 2019 Jul 5. Lancet HIV. 2019. PMID: 31285183 Free PMC article.
-
Using Predicted Cardiovascular Disease Risk in Conjunction With Blood Pressure to Guide Antihypertensive Medication Treatment.J Am Coll Cardiol. 2017 May 16;69(19):2446-2456. doi: 10.1016/j.jacc.2017.02.066. J Am Coll Cardiol. 2017. PMID: 28494981 Free PMC article. Review.
-
Using HIV Risk Prediction Tools to Identify Candidates for Pre-Exposure Prophylaxis: Perspectives from Patients and Primary Care Providers.AIDS Patient Care STDS. 2019 Aug;33(8):372-378. doi: 10.1089/apc.2019.0056. Epub 2019 Jun 17. AIDS Patient Care STDS. 2019. PMID: 31210551 Free PMC article.
-
Developing and validating clinical models to identify candidates for allergic rhinitis pre-exposure prophylaxis.Ann Med. 2023;55(2):2287188. doi: 10.1080/07853890.2023.2287188. Epub 2023 Dec 1. Ann Med. 2023. PMID: 38039557 Free PMC article.
References
-
- World Heatlh Organization Cardiovascular Diseases. http://www.who.int/mediacentre/factsheets/fs317/en/index.html.
-
- Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, Foster E, Hlatky MA, Hodgson JM, Kushner FG, Lauer MS, Shaw LJ, Smith SC Jr, Taylor AJ, Weintraub WS, Wenger NK. 2010 ACCF/AHA Guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines developed in collaboration with the American society of echocardiography, American society of nuclear cardiology, society of atherosclerosis imaging and prevention, society for cardiovascular angiography and interventions, society of cardiovascular computed tomography, and society for cardiovascular magnetic resonance. Journal of the American College of Cardiology 14. 2010;13:e50–e103. doi: 10.1016/j.jacc.2010.09.001. - DOI - PubMed
-
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation. 2002;13:3143–3143. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
