

Palm oil taxes and cardiovascular disease mortality in India: economic-epidemiologic model
- PMID: 24149818
- PMCID: PMC4688552
- DOI: 10.1136/bmj.f6048
Palm oil taxes and cardiovascular disease mortality in India: economic-epidemiologic model
Abstract
Objective: To examine the potential effect of a tax on palm oil on hyperlipidemia and on mortality due to cardiovascular disease in India.
Design: Economic-epidemiologic model.
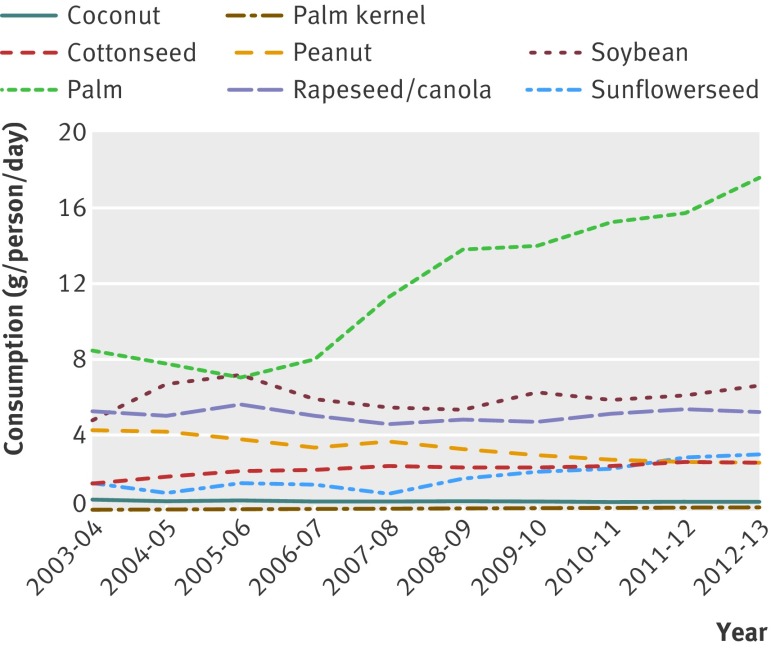
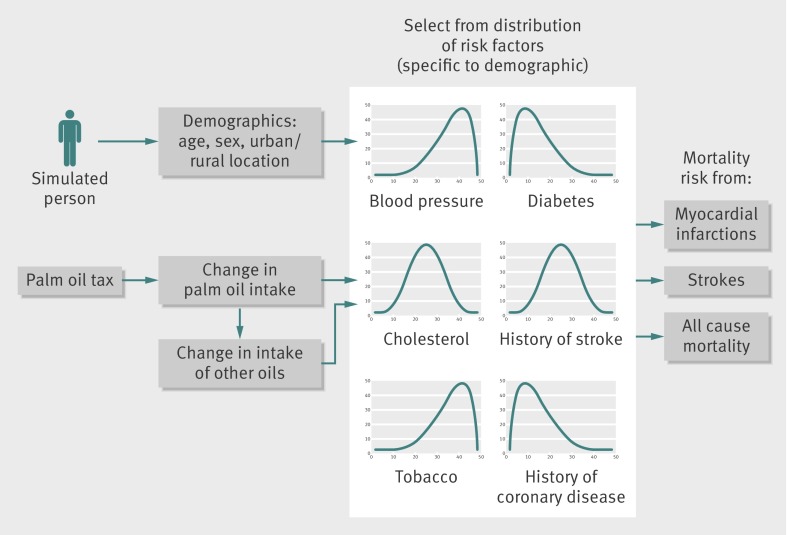
Modeling methods: A microsimulation model of mortality due to myocardial infarction and stroke among Indian populations was constructed, incorporating nationally representative data on systolic blood pressure, total cholesterol, tobacco smoking, diabetes, and cardiovascular event history, and stratified by age, sex, and urban/rural residence. Household expenditure data were used to estimate the change in consumption of palm oil following changes in oil price and the potential substitution of alternative oils that might occur after imposition of a tax. A 20% excise tax on palm oil purchases was simulated over the period 2014-23.
Main outcome measures: The model was used to project future mortality due to myocardial infarction and stroke, as well as the potential effect of a tax on food insecurity, accounting for the effect of increased food prices.
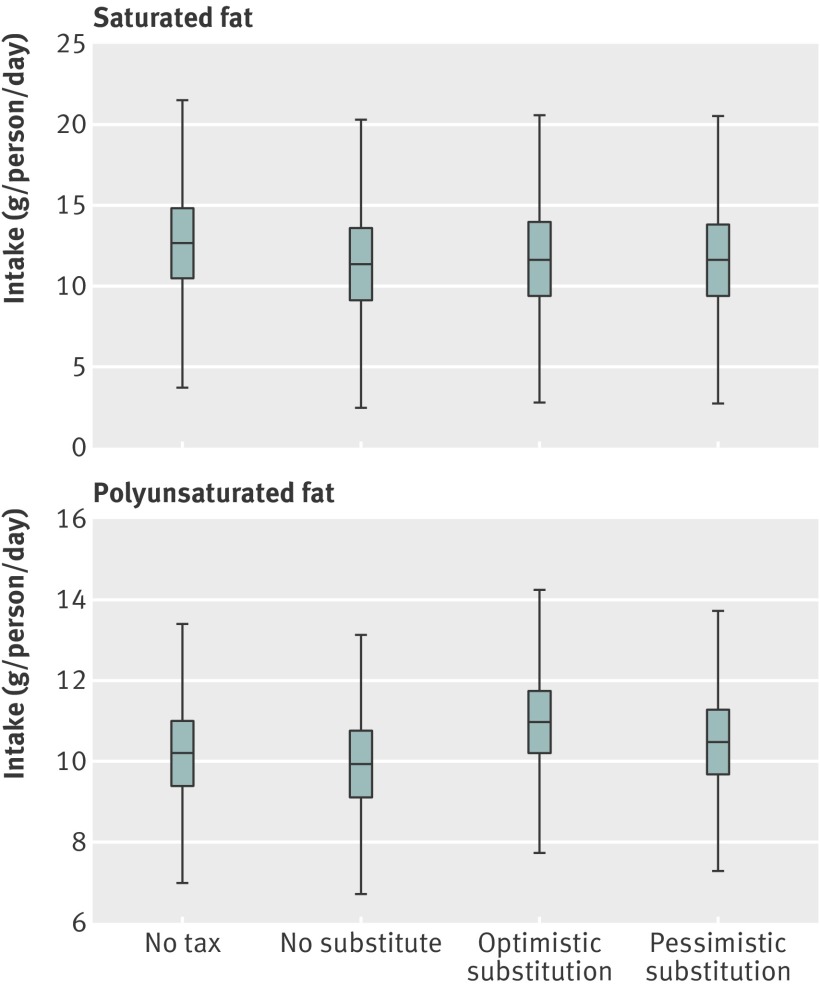
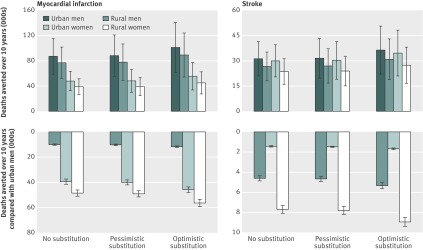
Results: A 20% tax on palm oil purchases would be expected to avert approximately 363,000 (95% confidence interval 247,000 to 479,000) deaths from myocardial infarctions and strokes over the period 2014-23 in India (1.3% reduction in cardiovascular deaths) if people do not substitute other oils for reduced palm oil consumption. Given estimates of substitution of palm oil with other oils following a 20% price increase for palm oil, the beneficial effects of increased polyunsaturated fat consumption would be expected to enhance the projected reduction in deaths to as much as 421,000 (256,000 to 586,000). The tax would be expected to benefit men more than women and urban populations more than rural populations, given differential consumption and cardiovascular risk. In a scenario incorporating the effect of taxation on overall food expenditures, the tax may increase food insecurity by <1%, resulting in 16,000 (95% confidence interval 12,000 to 22,000) deaths.
Conclusions: Curtailing palm oil intake through taxation may modestly reduce hyperlipidemia and cardiovascular mortality, but with potential distributional consequences differentially benefiting male and urban populations, as well as affecting food security.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
India has a problem with palm oil.BMJ. 2013 Oct 28;347:f6065. doi: 10.1136/bmj.f6065. BMJ. 2013. PMID: 24167201 No abstract available.
References
-
- Institute of Medicine. Promoting cardiovascular health in the developing world: a critical challenge to achieve global health. National Academy Press, 2010. - PubMed
-
- Alwan A. Global status report on noncommunicable diseases 2010. World Health Organization, 2011.
-
- Pearson TA. Cardiovascular disease in developing countries: myths, realities, and opportunities. Cardiovasc Drugs Ther 1999;13:95-104. - PubMed
-
- Mensink RP, Zock PL, Kester AD, Katan MB. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials. Am J Clin Nutr 2003;77:1146-55. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources