

Right hepatic lobe living donation: a 12 years single Italian center experience
- PMID: 24151353
- PMCID: PMC3801305
- DOI: 10.3748/wjg.v19.i38.6353
Right hepatic lobe living donation: a 12 years single Italian center experience
Abstract
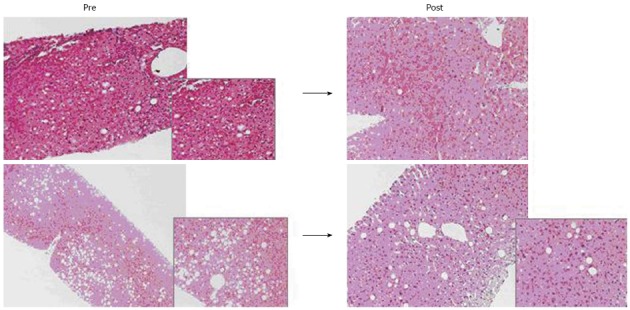
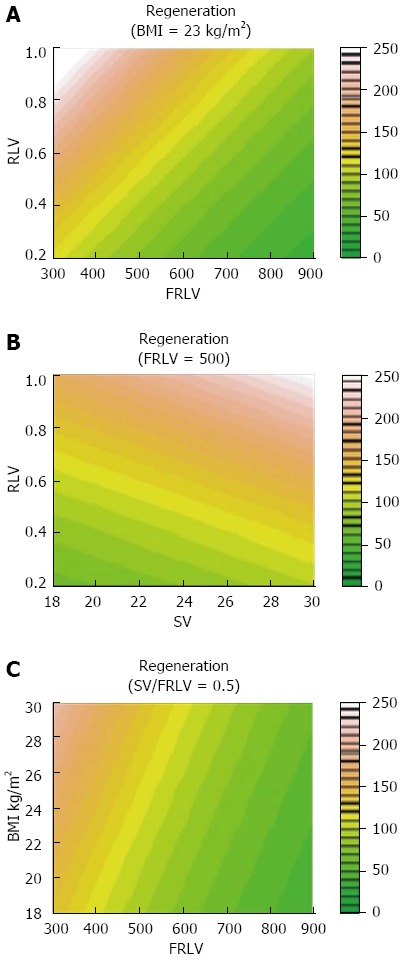
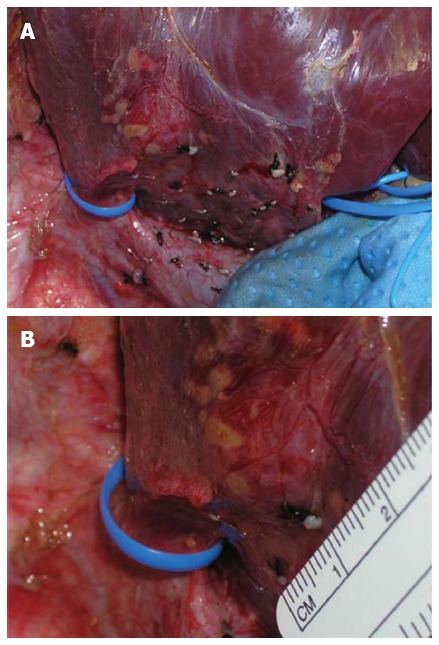
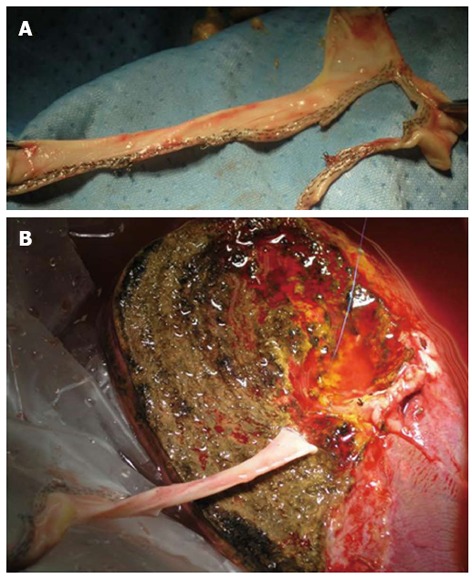
Mini invasive techniques are taking over conventional open liver resections in the setting of left lateral segmentectomy for living liver donation, and hydride procedure are being implemented for the living related right hepatectomy. Our center routinely performs laparoscopic left lateral segmentectomy for pediatric recipient and has been the first in the Europe performing an entirely robotic right hepatectomy. Great emphasis is posed on living donor safety which is the first priority during the entire operation, then the most majority of our procedures are still conventional open right hepatectomy (RHLD), defined as removal of a portion of liver corresponding to Couinaud segments 5-8, in order to obtain a graft for adult to adult living related liver transplant. During this 10 years period some changes, herein highlighted, have occurred to our surgical techniques. This study reports the largest Italian experience with RHLD, focused on surgical technique evolution over a 10 years period. Donor safety must be the first priority in right-lobe living-related donation: the categorization of complications of living donors, specially, after this "highly sensitive" procedure, reflects the need for prompt and detailed reports.
Keywords: Adult-to-adult living-related liver transplantation; Liver regeneration; Liver resections; Liver surgery; Liver transplantation.
Figures
References
-
- Gruttadauria S, Parikh V, Pagano D, Tuzzolino F, Cintorino D, Miraglia R, Spada M, Vizzini G, Luca A, Gridelli B. Early regeneration of the remnant liver volume after right hepatectomy for living donation: a multiple regression analysis. Liver Transpl. 2012;18:907–913. - PubMed
-
- Lortat-Jacob JL, ROBERT HG. [Well defined technic for right hepatectomy] Presse Med. 1952;60:549–551. - PubMed
-
- Gruttadauria S, Vasta F, Minervini MI, Piazza T, Arcadipane A, Marcos A, Gridelli B. Significance of the effective remnant liver volume in major hepatectomies. Am Surg. 2005;71:235–240. - PubMed
-
- Pagano D, Spada M, Grosso G, Cintorino D, Li Petri S, Luca A, Vizzini GB, Volpes R, Gridelli BG, Gruttadauria S. Impact of Donor’s Nutritional Status on Recipient Survival in a Consecutive Series of 87 Living-Related Liver Transplants. Liver Transpl. 2013;19:S273–S274.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
