

Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial
- PMID: 24153171
- PMCID: PMC3921966
- DOI: 10.1097/BRS.0000000000000088
Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial
Erratum in
- Spine (Phila Pa 1976). 2015 Jan;40(1):E59
Abstract
Study design: Concurrent prospective randomized and observational cohort studies.
Objective: To assess the 8-year outcomes of surgery versus nonoperative care.
Summary of background data: Although randomized trials have demonstrated small short-term differences in favor of surgery, long-term outcomes comparing surgical with nonoperative treatment remain controversial.
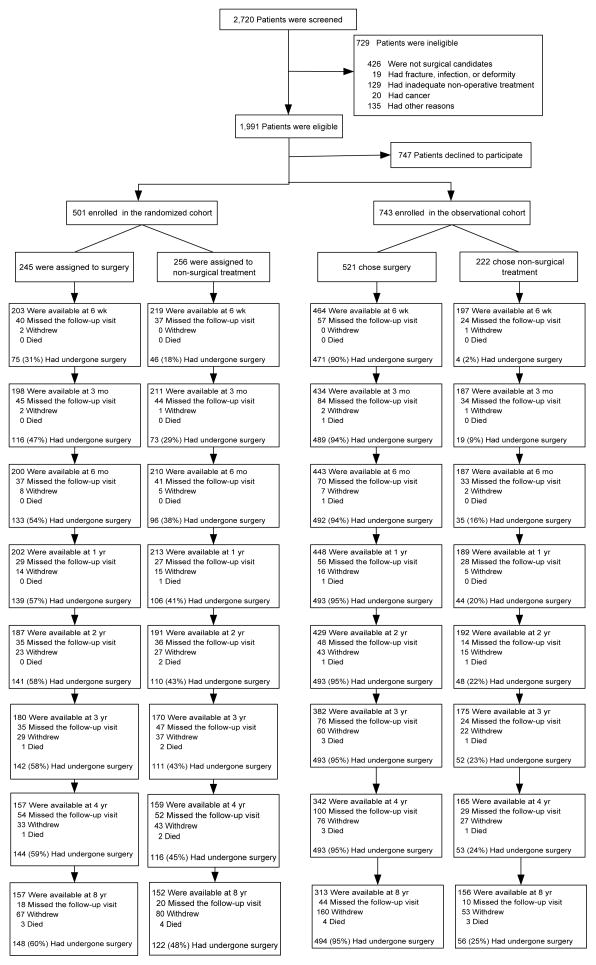
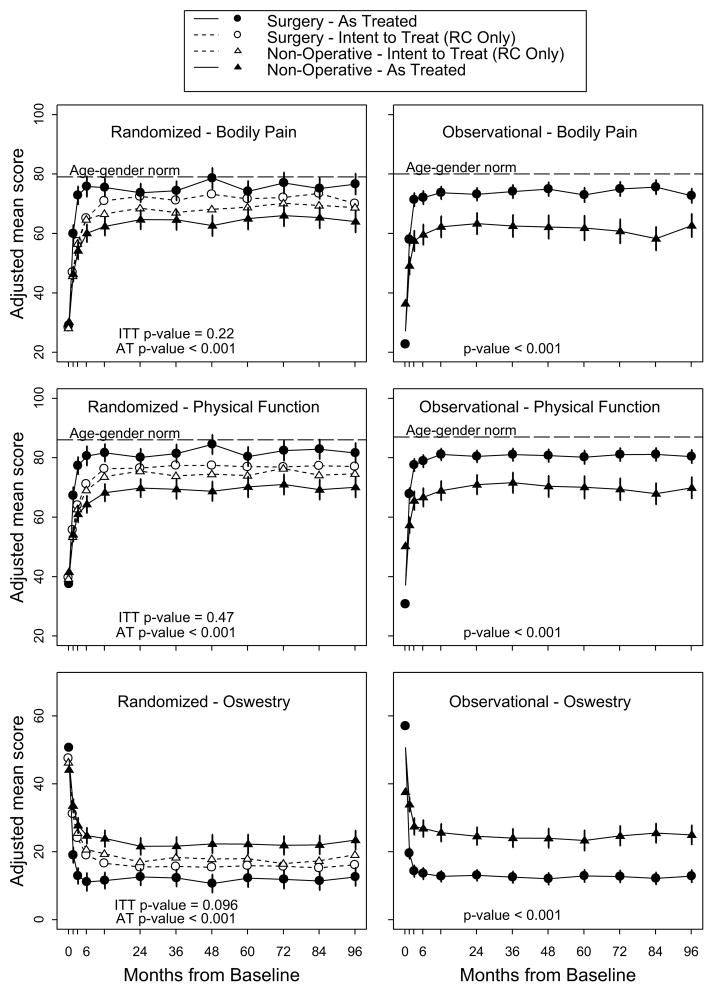
Methods: Surgical candidates with imaging-confirmed lumbar intervertebral disc herniation meeting Spine Patient Outcomes Research Trial eligibility criteria enrolled into prospective randomized (501 participants) and observational cohorts (743 participants) at 13 spine clinics in 11 US states. Interventions were standard open discectomy versus usual nonoperative care. Main outcome measures were changes from baseline in the SF-36 Bodily Pain and Physical Function scales and the modified Oswestry Disability Index-AAOS/Modems version assessed at 6 weeks, 3 months, and 6 months, and annually thereafter.
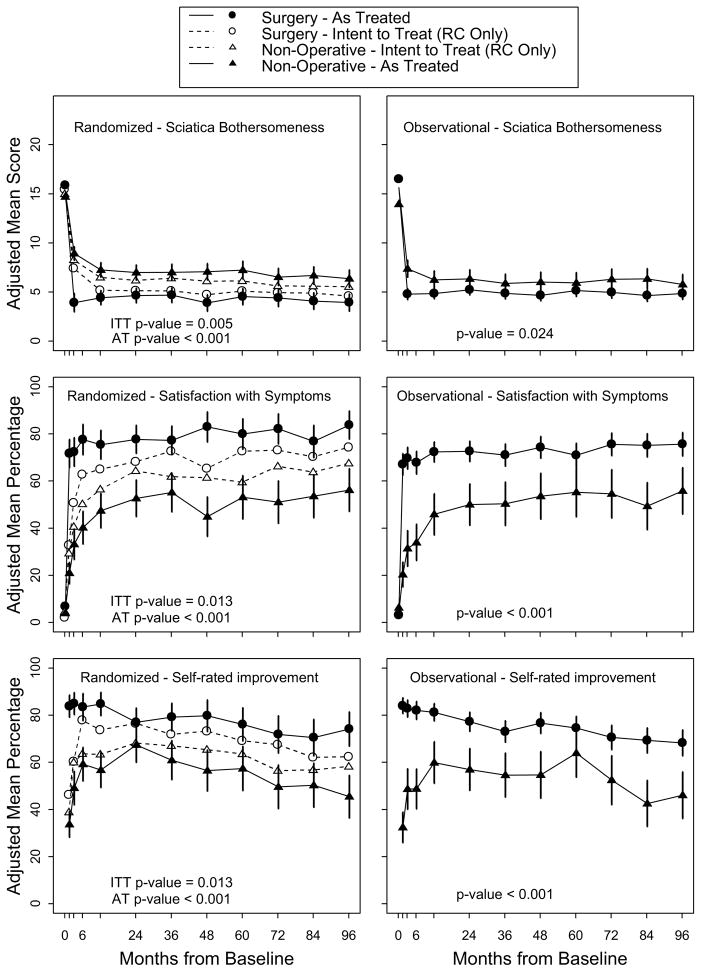
Results: Advantages were seen for surgery in intent-to-treat analyses for the randomized cohort for all primary and secondary outcomes other than work status; however, with extensive nonadherence to treatment assignment (49% patients assigned to nonoperative therapy receiving surgery versus 60% of patients assigned to surgery) these observed effects were relatively small and not statistically significant for primary outcomes (bodily pain, physical function, Oswestry Disability Index). Importantly, the overall comparison of secondary outcomes was significantly greater with surgery in the intent-to-treat analysis (sciatica bothersomeness [P > 0.005], satisfaction with symptoms [P > 0.013], and self-rated improvement [P > 0.013]) in long-term follow-up. An as-treated analysis showed significant surgical treatment effects for primary outcome measures (mean change, surgery vs. nonoperative care; treatment effect; 95% confidence interval): bodily pain (45.3 vs. 34.4; 10.9; 7.7 to 14); PF (42.2 vs. 31.5; 10.6; 7.7 to 13.5); and Oswestry Disability Index (-36.2 vs. -24.8; -11.3; -13.6 to -9.1).
Conclusion: Carefully selected patients who underwent surgery for a lumbar disc herniation achieved greater improvement than nonoperatively treated patients; there was little to no degradation of outcomes in either group (operative and nonoperative) from 4 to 8 years.
Level of evidence: 2.
Figures
Comment in
-
TO THE EDITOR.Spine (Phila Pa 1976). 2017 Oct 15;42(20):E1213-E1214. doi: 10.1097/BRS.0000000000002365. Spine (Phila Pa 1976). 2017. PMID: 28767633 No abstract available.
-
TO THE EDITOR.Spine (Phila Pa 1976). 2017 Oct 15;42(20):E1214. doi: 10.1097/BRS.0000000000002374. Spine (Phila Pa 1976). 2017. PMID: 28991874 Free PMC article. No abstract available.
References
-
- Dartmouth Atlas Working Group. Dartmouth Atlas of Musculoskeletal Health Care. Chicago, IL: American Hospital Association Press; 2000.
-
- Weber H. Lumbar disc herniation. A controlled, prospective study with ten years of observation. Spine. 1983;8:131–40. - PubMed
-
- Atlas SJ, Deyo RA, Keller RB, et al. The Maine Lumbar Spine Study, Part II. 1-year outcomes of surgical and nonsurgical management of sciatica. Spine. 1996;21:1777–86. - PubMed
-
- Peul WC, van Houwelingen HC, van den Hout WB, et al. Surgery versus prolonged conservative treatment for sciatica. N Engl J Med. 2007;356:2245–56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
