

A randomized, double-blind evaluation of buprenorphine taper duration in primary prescription opioid abusers
- PMID: 24153411
- PMCID: PMC4131728
- DOI: 10.1001/jamapsychiatry.2013.2216
A randomized, double-blind evaluation of buprenorphine taper duration in primary prescription opioid abusers
Abstract
Importance: Although abuse of prescription opioids (POs) is a significant public health problem, few experimental studies have investigated the treatment needs of this growing population.
Objective: To evaluate, following brief stabilization with a combination of buprenorphine hydrochloride and naloxone hydrochloride dihydrate, the relative efficacy of 1-, 2-, and 4-week buprenorphine tapering regimens and subsequent naltrexone hydrochloride therapy in PO-dependent outpatients.
Design, setting, and participants: A double-blind, 12-week randomized clinical trial was conducted in an outpatient research clinic. Following a brief period of buprenorphine stabilization, 70 PO-dependent adults were randomized to receive 1-, 2-, or 4-week tapers followed by naltrexone therapy.
Intervention: During phase 1 (weeks 1-5 after randomization), participants visited the clinic daily; during phase 2 (weeks 6-12), visits were reduced to thrice weekly. Participants received behavioral therapy and urine toxicology testing throughout the trial.
Main outcomes and measures: The percentage of participants negative for illicit opioid use, retention, naltrexone ingestion, and favorable treatment response (ie, retained in treatment, opioid abstinent, and receiving naltrexone at the end of the study).
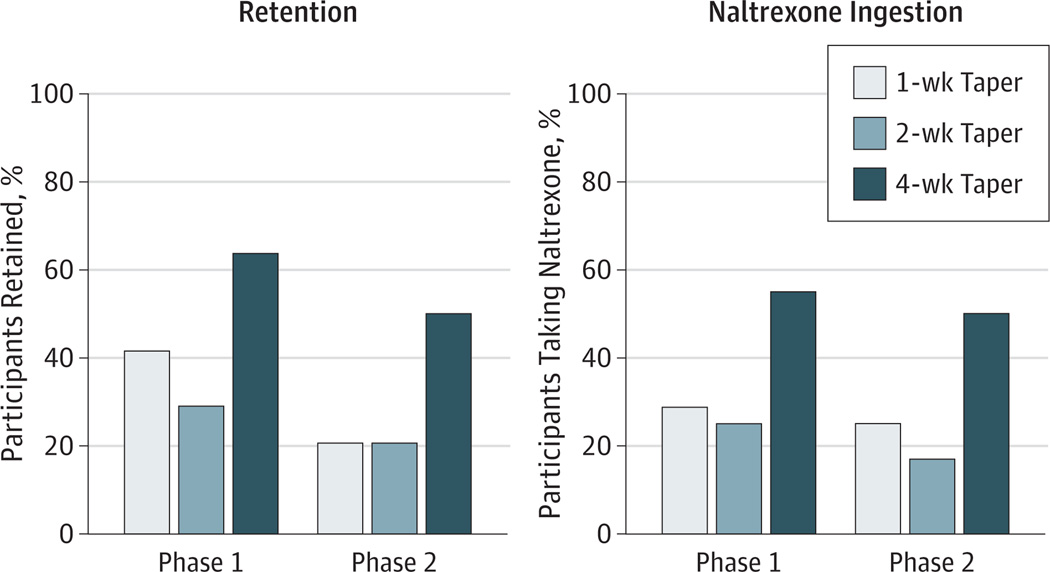
Results: Opioid abstinence at the end of phase 1 was greater in the 4-week compared with the 2- and 1-week taper conditions (P = .02), with 63% (n = 14), 29% (n = 7), and 29% (n = 7) of participants abstinent in the 4-, 2-, and 1-week conditions, respectively. Abstinence at the end of phase 2 was also greater in the 4-week compared with the 2- and 1-week conditions (P = .03), with 50% (n = 11), 16% (n = 4), and 20% (n = 5) of participants abstinent in the 4-, 2-, and 1-week conditions, respectively. There were more treatment responders in the 4-week condition (P = .03), with 50% (n = 11), 17% (n = 4), and 21% (n = 5) of participants in the 4-, 2-, and 1-week groups considered responders at the end of treatment, respectively. Retention and naltrexone ingestion also were superior in the 4-week vs briefer tapers (both P = .04). Experimental condition (ie, taper duration) was the strongest predictor of treatment response, followed by buprenorphine stabilization dose.
Conclusions and relevance: This study represents a rigorous experimental evaluation of outpatient buprenorphine stabilization, brief taper, and naltrexone maintenance for treatment of PO dependence. Results suggest that a meaningful subset of PO-dependent outpatients may respond positively to a 4-week taper plus naltrexone maintenance intervention.
Trial registration: ClinicalTrials.gov NCT00719095.
Conflict of interest statement
Figures



Comment in
-
Prescription opioid dependence: the clinical challenge.JAMA Psychiatry. 2014 Mar;71(3):338. doi: 10.1001/jamapsychiatry.2013.4530. JAMA Psychiatry. 2014. PMID: 24599244 No abstract available.
-
Treating prescription opioid dependence.JAMA. 2014 Sep 17;312(11):1145-6. doi: 10.1001/jama.2014.4318. JAMA. 2014. PMID: 25226480 No abstract available.
References
-
- Centers for Disease Control and Prevention (CDC) CDC grand rounds: prescription drug overdose—a U.S. epidemic. MMWR Morb Mortal Wkly Rep. 2012;61(1):10–13. - PubMed
-
- Compton WM, Volkow ND. Major increases in opioid analgesic abuse in the United States. Drug Alcohol Depend. 2006;81(2):103–107. - PubMed
-
- Maxwell JC. The prescription drug epidemic in the United States: a perfect storm. Drug Alcohol Rev. 2011;30(3):264–270. - PubMed
-
- Zacny J, Bigelow G, Compton P, Foley K, Iguchi M, Sannerud C. College on Problems of Drug Dependence taskforce on prescription opioid non-medical use and abuse: position statement. Drug Alcohol Depend. 2003;69(3):215–232. - PubMed
-
- Birnbaum HG, White AG, Reynolds JL, et al. Estimated costs of prescription opioid analgesic abuse in the United States in 2001: a societal perspective. Clin J Pain. 2006;22(8):667–676. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
