

Major cancer regressions in mesothelioma after treatment with an anti-mesothelin immunotoxin and immune suppression
- PMID: 24154601
- PMCID: PMC6369691
- DOI: 10.1126/scitranslmed.3006941
Major cancer regressions in mesothelioma after treatment with an anti-mesothelin immunotoxin and immune suppression
Abstract
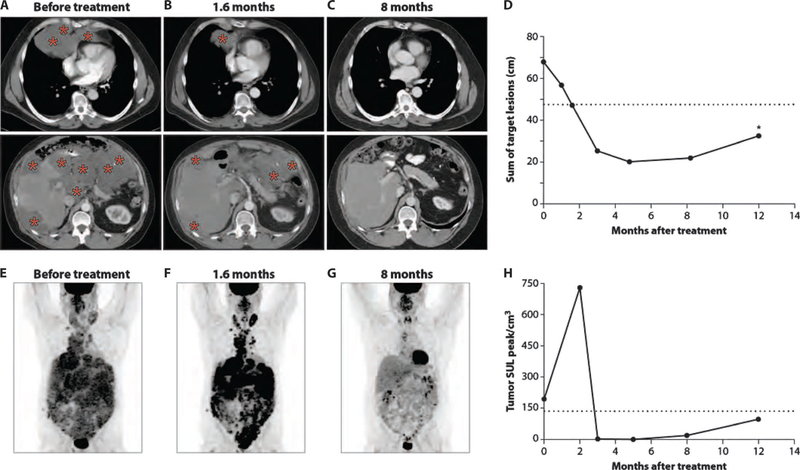
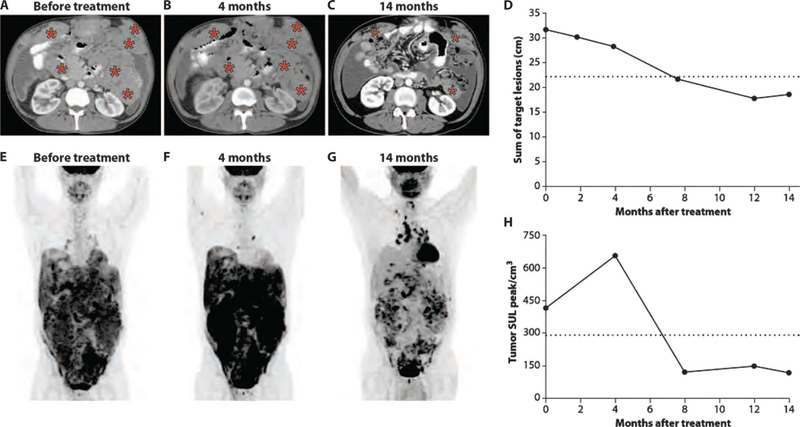
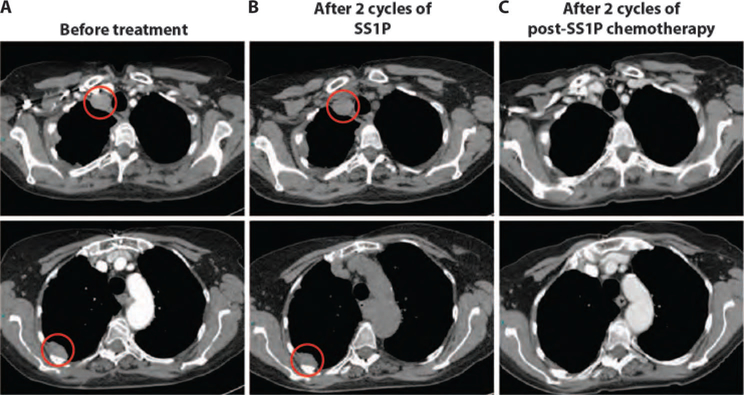
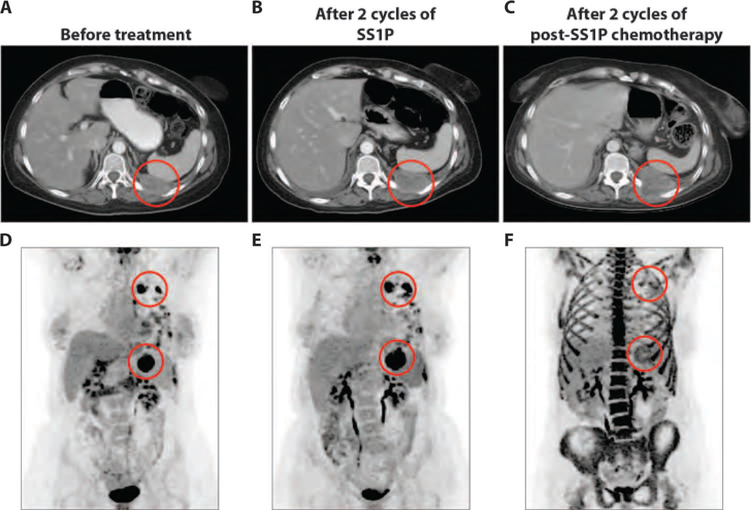
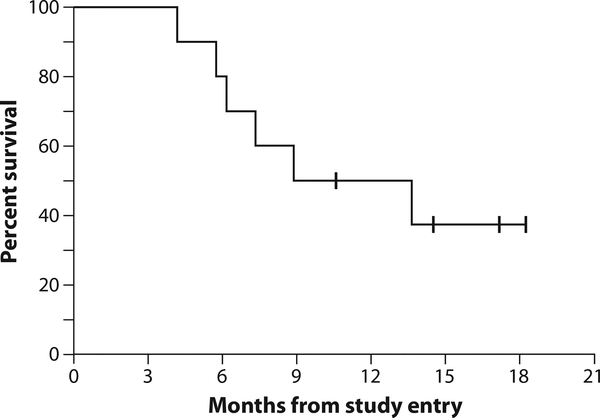
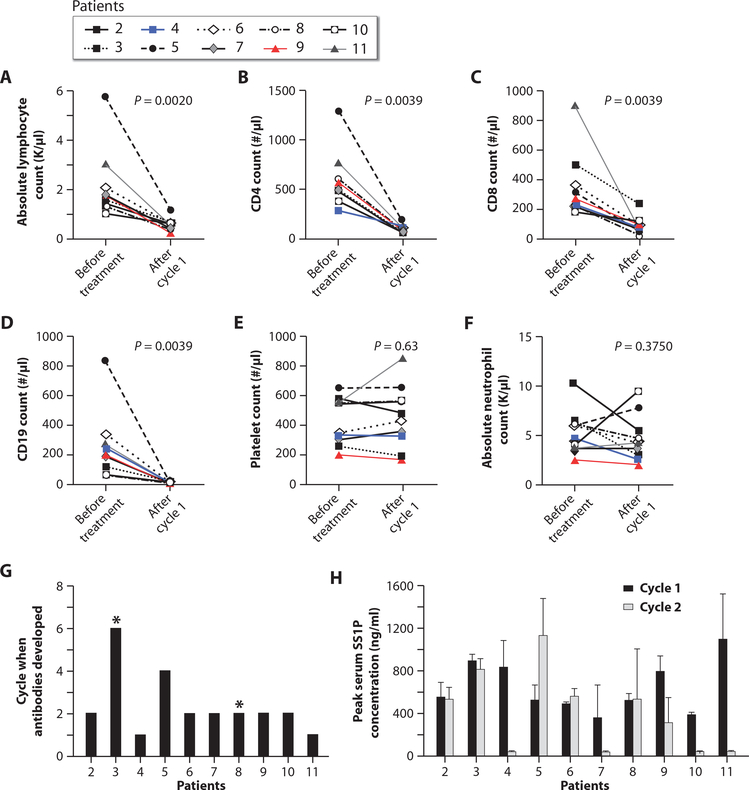
Immunotoxins are potent anticancer agents with an unusual mechanism of action: inhibition of protein synthesis resulting in apoptotic cell death. Immunotoxins have produced many durable complete responses in refractory hairy cell leukemia, where patients rarely form antibodies to the bacterial toxin component of the immunotoxin. Patients with mesothelioma, however, have normal immune systems and form antibodies after one cycle, and tumor responses to the immunotoxin have not been observed in this disease. We describe the results of a trial in which major antitumor responses were seen in patients with advanced mesothelioma who received the anti-mesothelin immunotoxin SS1P, together with pentostatin and cyclophosphamide, to deplete T and B cells. Of 10 patients with chemotherapy-refractory mesothelioma, 3 have had major tumor regressions with 2 ongoing at 15 months, and 2 others responded to chemotherapy after discontinuing immunotoxin therapy. Antibody formation was markedly delayed, allowing more SS1P cycles to be given, but this alone does not appear to account for the marked antitumor activity observed.
Conflict of interest statement
Figures


Comment in
-
A new hope for precision medicine.Sci Transl Med. 2013 Oct 23;5(208):208fs38. doi: 10.1126/scitranslmed.3007622. Sci Transl Med. 2013. PMID: 24154598
References
-
- Robinson BW, Lake RA, Advances in malignant mesothelioma. N. Engl. J. Med 353, 1591–1603 (2005). - PubMed
-
- Vogelzang NJ, Rusthoven JJ, Symanowski J, Denham C, Kaukel E, Ruffie P, Gatzemeier U,Boyer M, Emri S, Manegold C, Niyikiza C, Paoletti P, Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J. Clin. Oncol 21, 2636–2644 (2003). - PubMed
-
- Yan TD, Deraco M, Baratti D, Kusamura S, Elias D, Glehen O, Gilly FN, Levine EA, Shen P,Mohamed F, Moran BJ, Morris DL, Chua TC, Piso P, Sugarbaker PH, Cytoreductive surgery and hyperthermic intaperitoneal chemotherapy for malignant peritoneal mesothelioma: Multi-institutional experience. J. Clin. Oncol 27, 6237–6242 (2009). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
