

Multiportal robotic access to the anterior cranial fossa: a surgical and engineering feasibility study
- PMID: 24154747
- PMCID: PMC5953425
- DOI: 10.1177/0194599813509587
Multiportal robotic access to the anterior cranial fossa: a surgical and engineering feasibility study
Abstract
Objective: Integration of robotic surgical technology into skull base surgery is limited due to minimum angle requirements between robotic tools (narrow funnel effect), steep angle of approach, and instrumentation size. The objectives of this study were to systematically analyze surgical approach portals using a computer model, determine optimal approaches, and assess feasibility of the derived approaches on robotic surgical systems.
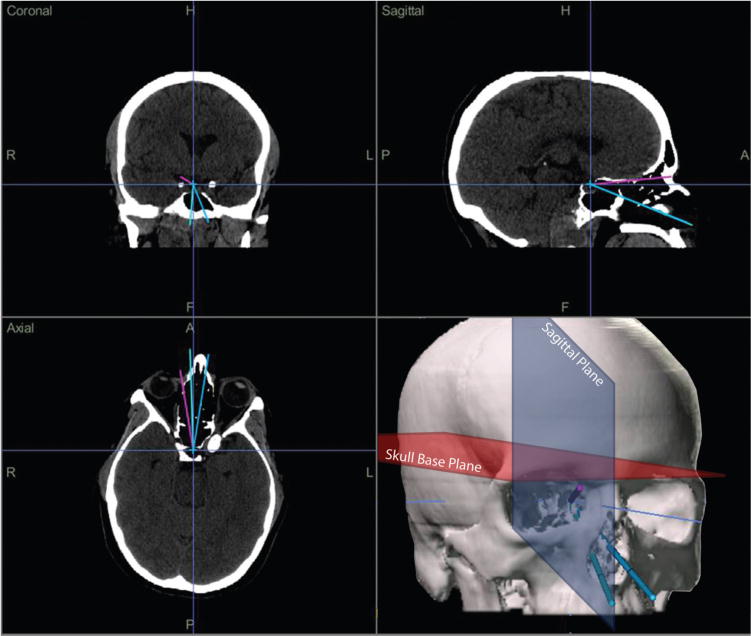
Study design: Computer analysis on 10 computed tomography scans was performed to determine approach trajectories, angles between robotic tools, and distances to specified skull base target locations for transorbital and transnasal surgical approach portals.
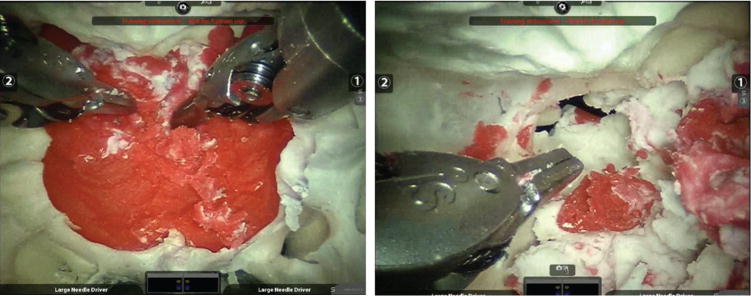
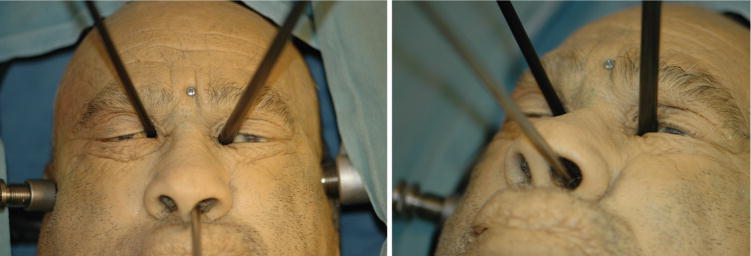
Setting: Dry laboratory and cadaver laboratory.
Subjects and methods: The optimal combinations were tested on the da Vinci and Raven robotic systems.
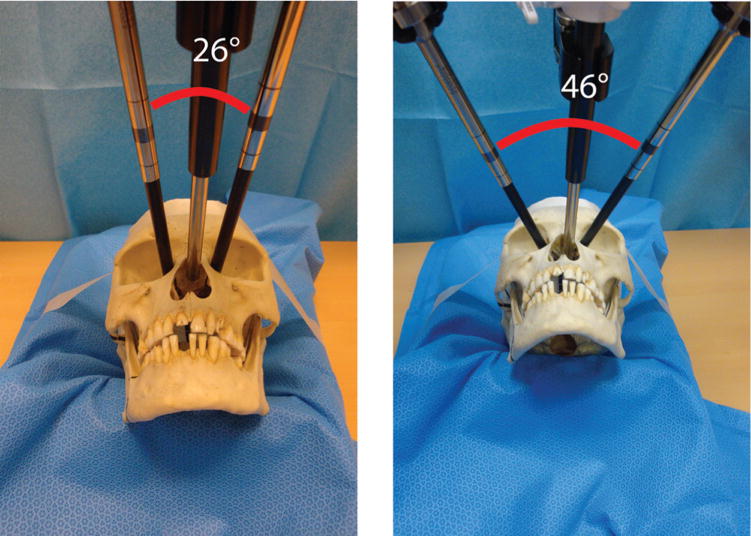
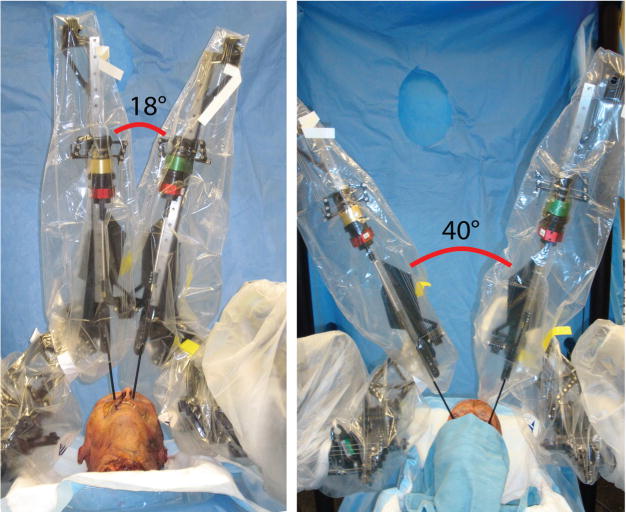
Results: Multiportal analyses showed the angles between 2 robotic tools were 14.7, 28.3, and 52.0 degrees in the cases of 2 transnasal portals, combined transnasal and medial orbit portals, and bilateral superior orbit portals, respectively, approaching a prechiasmatic target. The addition of medial and superior transorbital portals improved the skull base trajectory angles 21 and 27 degrees, respectively. Two robotic tools required an angle of at least 20 degrees between them to function effectively at skull base targets.
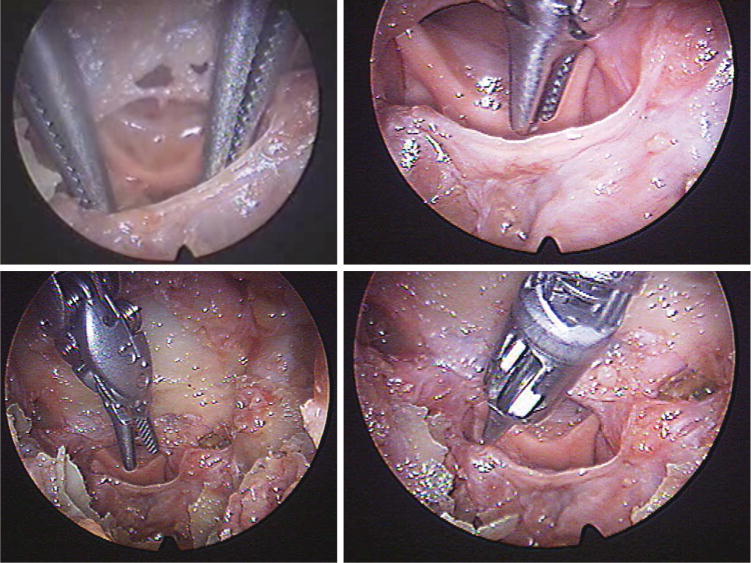
Conclusion: Technical feasibility of robotic transorbital and transnasal approaches to access sella and parasellar target locations was demonstrated. This technique addresses the 2 major drawbacks of (1) the narrow funnel effect generated from portals in close proximity and (2) the steep angle of approach to the skull base, as observed in previous studies analyzing transoral, transcervical, transmaxillary, and transhyoid portals.
Keywords: endoscopic; pituitary; robotic surgery; skull base; transorbital.
Conflict of interest statement
Figures
References
-
- Hanna EY, Holsinger C, DeMonte F, Kupferman M. Robotic endoscopic surgery of the skull base: a novel surgical approach. Arch Otolaryngol Head Neck Surg. 2007;133:1209–1214. - PubMed
-
- McCool RR, Warren FM, Wiggins RH, III, Hunt JP. Robotic surgery of the infratemporal fossa utilizing novel suprahyoid port. Laryngoscope. 2010;120:1738–1743. - PubMed
-
- O’Malley BW, Weinstein GS. Robotic anterior and midline skull base surgery: preclinical investigations. Int J Radiat Oncol Biol Phys. 2007;69(suppl 2):S125–S128. - PubMed
-
- Lee JY, O’Malley BW, Jr, Newman JG, et al. Transoral robotic surgery of the skull base: a cadaver and feasibility study. ORL J Otorhinolaryngol Relat Spec. 2010;72:181–187. - PubMed
-
- Kupferman M, Demonte F, Holsinger FC, et al. Transantral robotic access to the pituitary gland. Otolaryngol Head Neck Surg. 2009;141:413–415. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
