

State parity laws and access to treatment for substance use disorder in the United States: implications for federal parity legislation
- PMID: 24154931
- PMCID: PMC4047825
- DOI: 10.1001/jamapsychiatry.2013.2169
State parity laws and access to treatment for substance use disorder in the United States: implications for federal parity legislation
Abstract
Importance: The passage of the 2008 Mental Health Parity and Addiction Equity Act and the 2010 Affordable Care Act incorporated parity for substance use disorder (SUD) treatment into federal legislation. However, prior research provides us with scant evidence as to whether federal parity legislation will hold the potential for improving access to SUD treatment.
Objective: To examine the effect of state-level SUD parity laws on state-aggregate SUD treatment rates and to shed light on the impact of the recent federal SUD parity legislation.
Design, setting, and participants: We conducted a quasi-experimental study using a 2-way (state and year) fixed-effect method. We included all known specialty SUD treatment facilities in the United States and examined treatment rates from October 1, 2000, through March 31, 2008. Our main source of data was the National Survey of Substance Abuse Treatment Services, which provides facility-level information on specialty SUD treatment.
Interventions: State-level SUD parity laws during the study period.
Main outcomes and measures: State-aggregate SUD treatment rates in (1) all specialty SUD treatment facilities and (2) specialty SUD treatment facilities accepting private insurance.
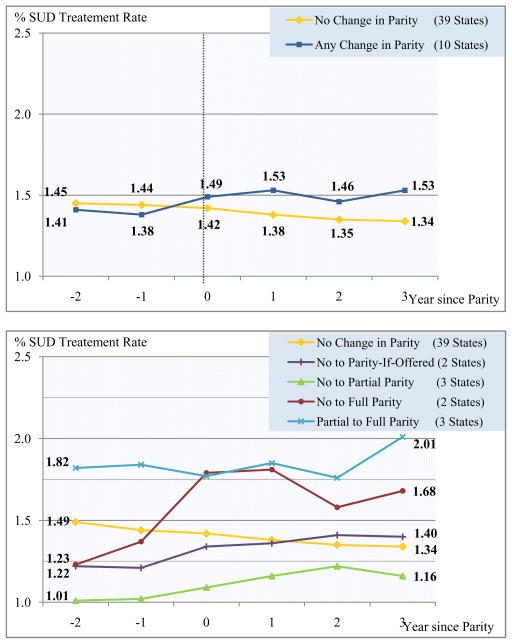
Results: The implementation of any SUD parity law increased the treatment rate by 9% (P < .001) in all specialty SUD treatment facilities and by 15% (P = .02) in facilities accepting private insurance. Full parity and parity only if SUD coverage is offered increased the SUD treatment rate by 13% (P = .02) and 8% (P = .04), respectively, in all facilities and by 21% (P = .03) and 10% (P = .04), respectively, in facilities accepting private insurance.
Conclusions and relevance: We found a positive effect of the implementation of state SUD parity legislation on access to specialty SUD treatment. Furthermore, the positive association is more pronounced in states with more comprehensive parity laws. Our findings suggest that federal parity legislation holds the potential to improve access to SUD treatment.
Conflict of interest statement
Figures
References
-
- United States. Substance Abuse and Mental Health Services Administration. Results from the 2010 National Survey on Drug Use and Health: summary of national findings. Rockville, MD: U.S. Dept. of Health and Human Services Substance Abuse and Mental Health Services Administration Center for Behaviorial Health Statistics and Quality; 2011.
-
- Winklbaur B, Jagsch R, Ebner N, Thau K, Fischer G. Quality of life in patients receiving opioid maintenance therapy. European addiction research. 2008;14(2):99–105. - PubMed
-
- Roux P, Carrieri MP, Villes V, Dellamonica P, Poizot-Martin I, Ravaux I, et al. The impact of methadone or buprenorphine treatment and ongoing injection on highly active antiretroviral therapy (HAART) adherence: evidence from the MANIF2000 cohort study. Addiction. 2008;103(11):1828–36. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
