

Psychosocial interventions for supporting women to stop smoking in pregnancy
- PMID: 24154953
- PMCID: PMC4022453
- DOI: 10.1002/14651858.CD001055.pub4
Psychosocial interventions for supporting women to stop smoking in pregnancy
Update in
-
Psychosocial interventions for supporting women to stop smoking in pregnancy.Cochrane Database Syst Rev. 2017 Feb 14;2(2):CD001055. doi: 10.1002/14651858.CD001055.pub5. Cochrane Database Syst Rev. 2017. PMID: 28196405 Free PMC article.
Abstract
Background: Tobacco smoking in pregnancy remains one of the few preventable factors associated with complications in pregnancy, stillbirth, low birthweight and preterm birth and has serious long-term implications for women and babies. Smoking in pregnancy is decreasing in high-income countries, but is strongly associated with poverty and increasing in low- to middle-income countries.
Objectives: To assess the effects of smoking cessation interventions during pregnancy on smoking behaviour and perinatal health outcomes.
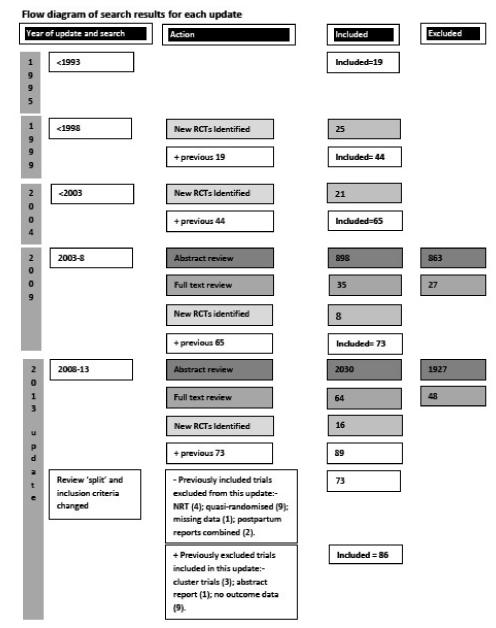
Search methods: In this fifth update, we searched the Cochrane Pregnancy and Childbirth Group's Trials Register (1 March 2013), checked reference lists of retrieved studies and contacted trial authors to locate additional unpublished data.
Selection criteria: Randomised controlled trials, cluster-randomised trials, randomised cross-over trials, and quasi-randomised controlled trials (with allocation by maternal birth date or hospital record number) of psychosocial smoking cessation interventions during pregnancy.
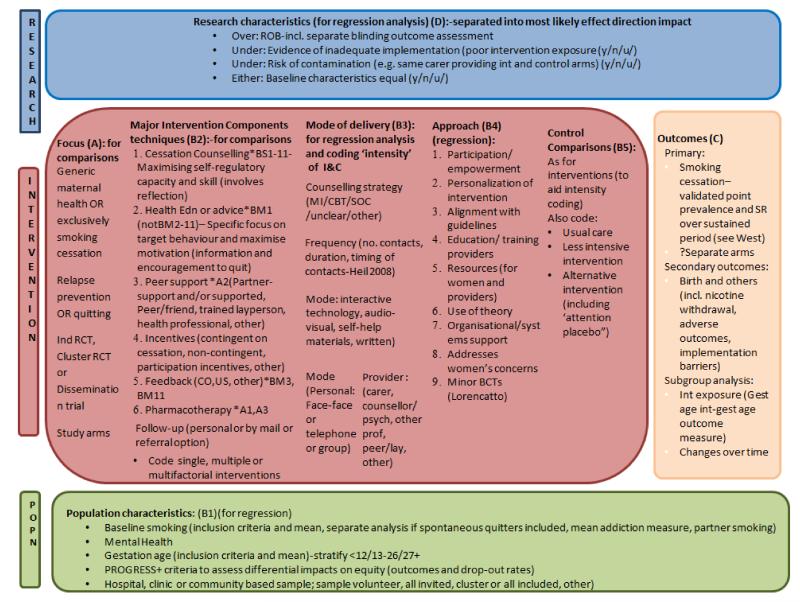
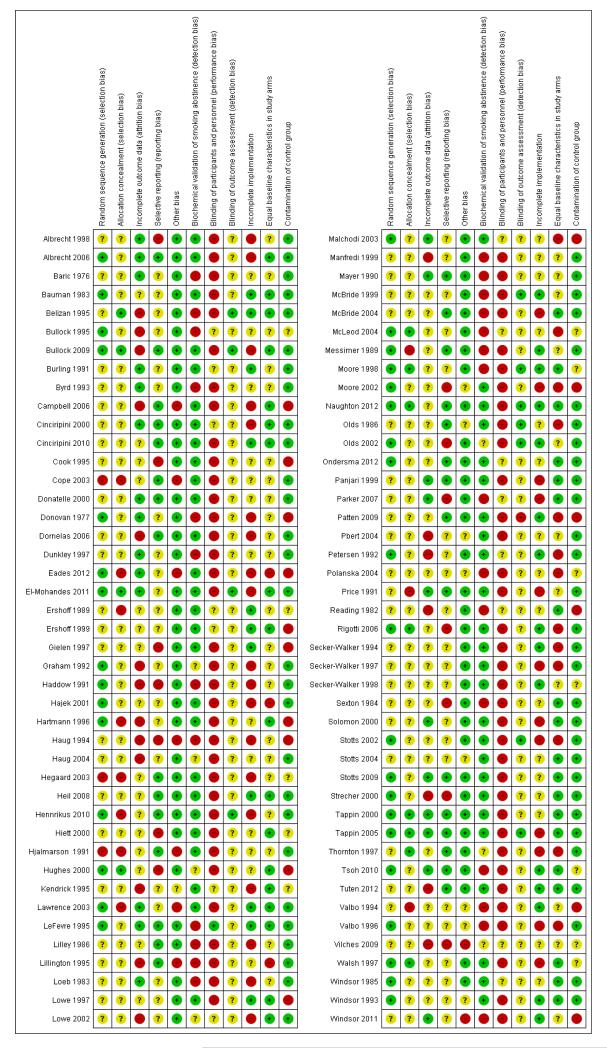
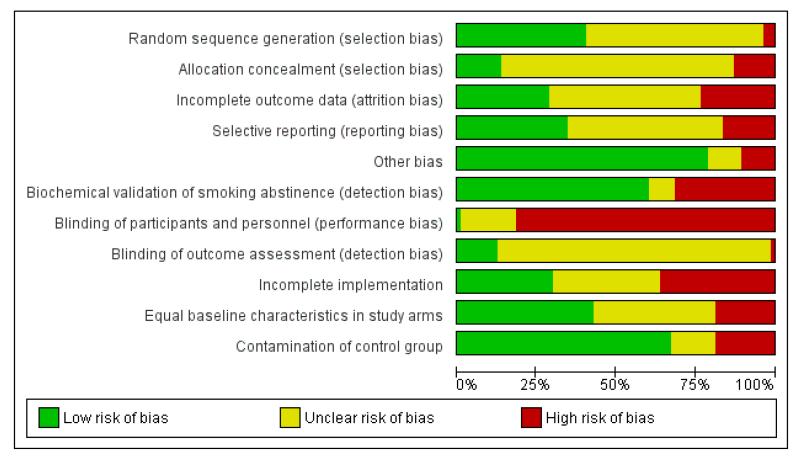
Data collection and analysis: Two review authors independently assessed trials for inclusion and trial quality, and extracted data. Direct comparisons were conducted in RevMan, and subgroup analyses and sensitivity analysis were conducted in SPSS.
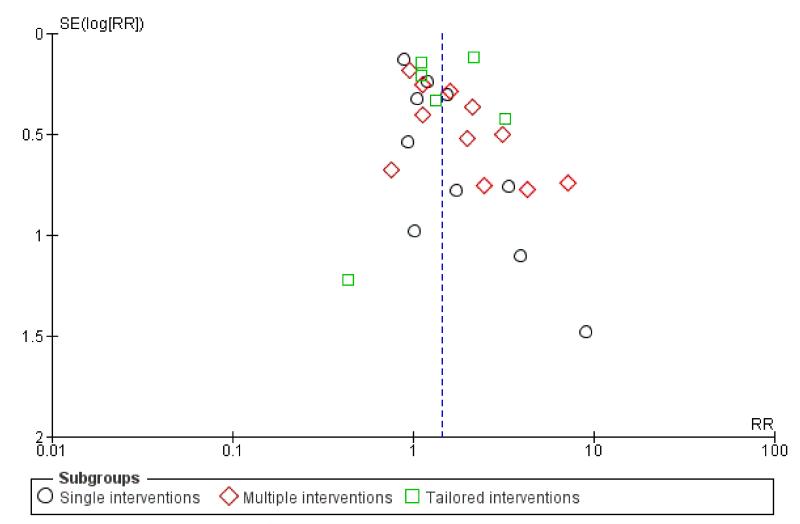
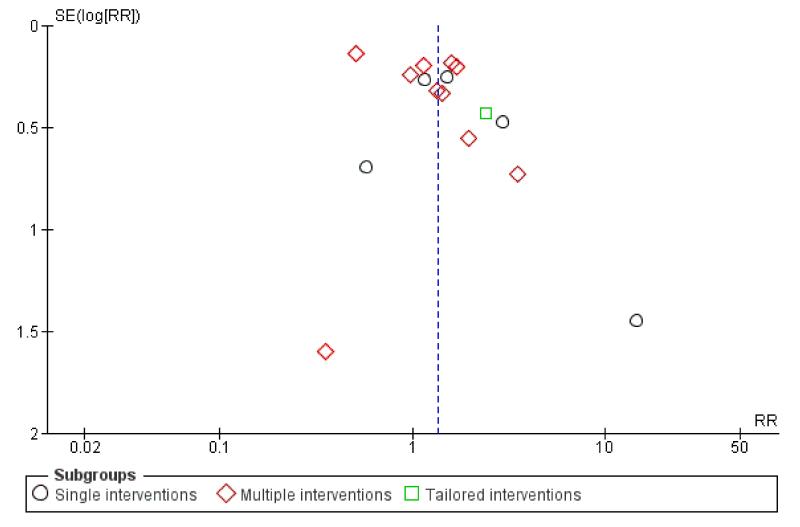
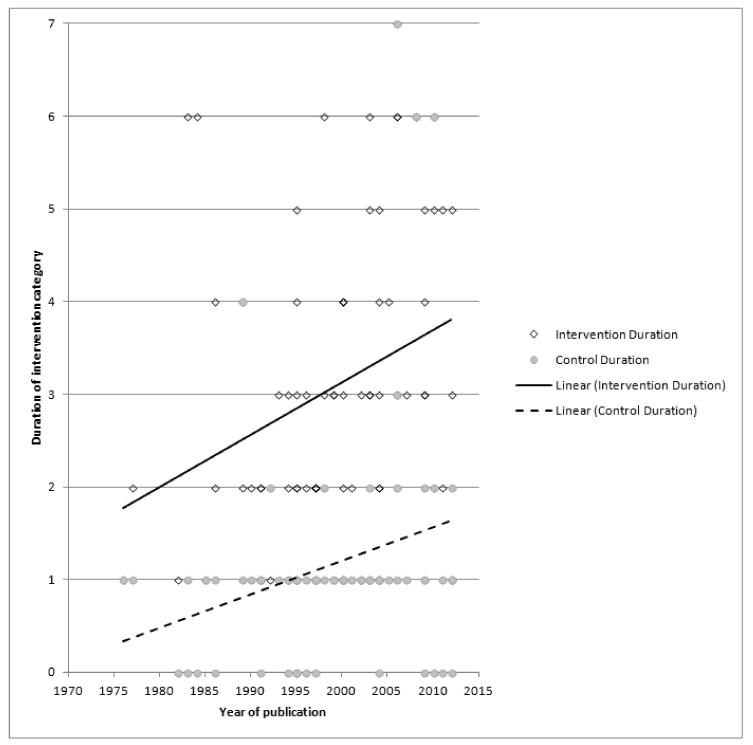
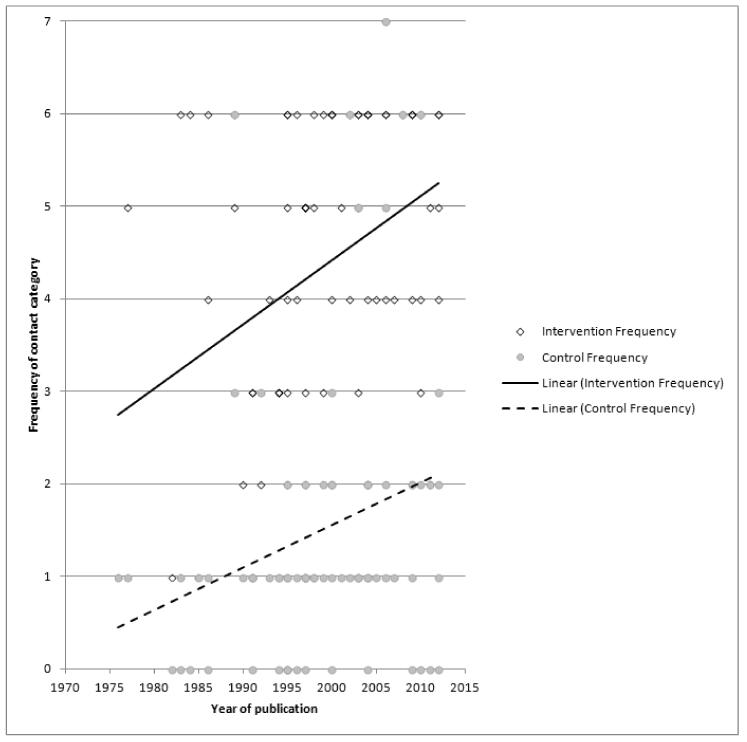
Main results: Eighty-six trials were included in this updated review, with 77 trials (involving over 29,000 women) providing data on smoking abstinence in late pregnancy.In separate comparisons, counselling interventions demonstrated a significant effect compared with usual care (27 studies; average risk ratio (RR) 1.44, 95% confidence interval (CI) 1.19 to 1.75), and a borderline effect compared with less intensive interventions (16 studies; average RR 1.35, 95% CI 1.00 to 1.82). However, a significant effect was only seen in subsets where counselling was provided in conjunction with other strategies. It was unclear whether any type of counselling strategy is more effective than others (one study; RR 1.15, 95% CI 0.86 to 1.53). In studies comparing counselling and usual care (the largest comparison), it was unclear whether interventions prevented smoking relapse among women who had stopped smoking spontaneously in early pregnancy (eight studies; average RR 1.06, 95% CI 0.93 to 1.21). However, a clear effect was seen in smoking abstinence at zero to five months postpartum (10 studies; average RR 1.76, 95% CI 1.05 to 2.95), a borderline effect at six to 11 months (six studies; average RR 1.33, 95% CI 1.00 to 1.77), and a significant effect at 12 to 17 months (two studies, average RR 2.20, 95% CI 1.23 to 3.96), but not in the longer term. In other comparisons, the effect was not significantly different from the null effect for most secondary outcomes, but sample sizes were small.Incentive-based interventions had the largest effect size compared with a less intensive intervention (one study; RR 3.64, 95% CI 1.84 to 7.23) and an alternative intervention (one study; RR 4.05, 95% CI 1.48 to 11.11).Feedback interventions demonstrated a significant effect only when compared with usual care and provided in conjunction with other strategies, such as counselling (two studies; average RR 4.39, 95% CI 1.89 to 10.21), but the effect was unclear when compared with a less intensive intervention (two studies; average RR 1.19, 95% CI 0.45 to 3.12).The effect of health education was unclear when compared with usual care (three studies; average RR 1.51, 95% CI 0.64 to 3.59) or less intensive interventions (two studies; average RR 1.50, 95% CI 0.97 to 2.31).Social support interventions appeared effective when provided by peers (five studies; average RR 1.49, 95% CI 1.01 to 2.19), but the effect was unclear in a single trial of support provided by partners.The effects were mixed where the smoking interventions were provided as part of broader interventions to improve maternal health, rather than targeted smoking cessation interventions.Subgroup analyses on primary outcome for all studies showed the intensity of interventions and comparisons has increased over time, with higher intensity interventions more likely to have higher intensity comparisons. While there was no significant difference, trials where the comparison group received usual care had the largest pooled effect size (37 studies; average RR 1.34, 95% CI 1.25 to 1.44), with lower effect sizes when the comparison group received less intensive interventions (30 studies; average RR 1.20, 95% CI 1.08 to 1.31), or alternative interventions (two studies; average RR 1.26, 95% CI 0.98 to 1.53). More recent studies included in this update had a lower effect size (20 studies; average RR 1.26, 95% CI 1.00 to 1.59), I(2)= 3%, compared to those in the previous version of the review (50 studies; average RR 1.50, 95% CI 1.30 to 1.73). There were similar effect sizes in trials with biochemically validated smoking abstinence (49 studies; average RR 1.43, 95% CI 1.22 to 1.67) and those with self-reported abstinence (20 studies; average RR 1.48, 95% CI 1.17 to 1.87). There was no significant difference between trials implemented by researchers (efficacy studies), and those implemented by routine pregnancy staff (effectiveness studies), however the effect was unclear in three dissemination trials of counselling interventions where the focus on the intervention was at an organisational level (average RR 0.96, 95% CI 0.37 to 2.50). The pooled effects were similar in interventions provided for women with predominantly low socio-economic status (44 studies; average RR 1.41, 95% CI 1.19 to 1.66), compared to other women (26 studies; average RR 1.47, 95% CI 1.21 to 1.79); though the effect was unclear in interventions among women from ethnic minority groups (five studies; average RR 1.08, 95% CI 0.83 to 1.40) and aboriginal women (two studies; average RR 0.40, 95% CI 0.06 to 2.67). Importantly, pooled results demonstrated that women who received psychosocial interventions had an 18% reduction in preterm births (14 studies; average RR 0.82, 95% CI 0.70 to 0.96), and infants born with low birthweight (14 studies; average RR 0.82, 95% CI 0.71 to 0.94). There did not appear to be any adverse effects from the psychosocial interventions, and three studies measured an improvement in women's psychological wellbeing.
Authors' conclusions: Psychosocial interventions to support women to stop smoking in pregnancy can increase the proportion of women who stop smoking in late pregnancy, and reduce low birthweight and preterm births.
Figures
Update of
-
Interventions for promoting smoking cessation during pregnancy.Cochrane Database Syst Rev. 2009 Jul 8;(3):CD001055. doi: 10.1002/14651858.CD001055.pub3. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2013 Oct 23;(10):CD001055. doi: 10.1002/14651858.CD001055.pub4. PMID: 19588322 Free PMC article. Updated.
References
References to studies included in this review
-
- Albrecht S, Cassidy B, Salamie D, Reynolds M. What’s happening. A smoking cessation intervention for pregnant adolescents: implications for nurse practitioners. Journal of American Academy of Nurse Practitioners. 1999;11(4):155–9. - PubMed
- Albrecht S, Cornelius M, Braxter B, Reynolds M, Stone C, Cassidy B. An assessment of nicotine dependence among pregnant adolescents. Journal of Substance Abuse Treatment. 1999;16(4):337–44. - PubMed
- Albrecht S, Stone CA, Payne L, Reynolds MD. A preliminary study of the use of peer support in smoking cessation programs for pregnant adolescents. Journal of the American Academy of Nurse Practitioners. 1998;10:119–25. - PubMed
- Albrecht SA, Higgins LW, Stone C. Factors relating to pregnant adolescents’ decisions to complete a smoking cessation intervention. Journal of Pediatric Nursing. 1999;14(5):322–8. - PubMed
-
- Albrecht SA, Caruthers D. Characteristics of inner-city pregnant Smoking teenagers. Journal of Obstetric Gynecologic and Neonatal Nursing. 2002;31:462–9. - PubMed
- Albrecht SA, Caruthers D, Patrick T, Reynolds M, Salamie D, Higgins LW, et al. A randomised controlled trial of a smoking cessation intervention for pregnant adolescents. Nursing Research. 2006;55(6):402–10. - PubMed
- Albrecht SA, Higgins LW, Lebow H. Knowledge about the deletrious effects of smoking and its relationship to smoking cessation among pregnant adolescents. Adolescence. 2000;35(140):709–16. - PubMed
- Albrecht SA, Patrick T, Kim Y, Caruthers D. A randomised controlled trial of a smoking cessation intervention for pregnant adolescents. Society for Research on Nicotine and Tobacco 9th Annual Meeting; New Orleans, Louisiana. 2003 February 19-23.2003. p. 91.
-
- Belizan JM, Villar J, Victora C, Farnot U, Langer A, Barros F. Impact of health education during pregnancy on behavior and utilization of health resources. American Journal of Obstetrics and Gynecology. 1995;173:894–9. - PubMed
- Victora CG, Langer A, Barros F, Belizan J, Farnot U, Villar J, et al. The Latin American Multicenter Trial on psychosocial support during pregnancy: methodology and baseline comparability. Controlled Clinical Trials. 1994;15:379–94. - PubMed
- Villar J, Farnot U, Barros F, Victora C, Langer A, Belizan JM. A randomized trial of psychosocial support during high-risk pregnancies. New England Journal of Medicine. 1992;327:1266–71. - PubMed
References to studies excluded from this review
-
- Albrecht S, Kelly-Thomas K, Osborne JW, Ogbagaber S. The SUCCESS program for smoking cessation for pregnant women. Journal of Obstetric Gynecologic and Neonatal Nursing. 2011;40:520–31. - PubMed
-
- Andrews JO, Bentley G, Crawford S, Pretlow L, Tingen MS. Using community-based participatory research to develop a culturally sensitive smoking cessation intervention with public housing neighbourhoods. Ethnicity and Disease. 2007;17:326–31. - PubMed
- Andrews JO, Felton G, Wewers ME, Waller J, Tingen M. The effect of a multi-component smoking cessation intervention in African American women residing in public housing. Research in Nursing and Health. 2007;30:45–60. - PubMed
-
- Berlin I. Study of Nicotine Patch in Pregnancy (SNIPP) ClinicalTrials.gov. 2008.
-
- Boshier A, Wilton LV, Shakir SAW. Evaluation of the safety of bupropion (Zyban) for smoking cessation from experience gained in general practice use in England in 2000. European Journal of Clinical Pharmacology. 2003;59:767–73. - PubMed
-
- Bowden JA, Oag DA, Smith KL, Miller CI. An integrated brief intervention to address smoking in pregnancy. Acta Obstetricia et Gynecologica. 2010;89:496–504. - PubMed
References to ongoing studies
-
- Althabe F, Berrueta M, Mazzoni A, Morello P, Aleman A, Colomar M. Prenatal tobacco cessation intervention for women in Latin America. International Journal of Gynecology and Obstetrics. 2012;119(Suppl 3):S165.
-
- Blasco Oliete M, Sanz Cuesta T, Girbés Fontana M, Pascual Malanda M, Ortiz Valdepeñas J, Garcia Lopez L. Effectiveness of two health interventions to get pregnant women to give up smoking [Efectividad de dos intervenciones sanitarias para conseguir el abandono del consumo de tabaco.] Atencion Primaria. 2004;33(5):277–83. - PMC - PubMed
-
- Everett KD, Debnam KJ, Gwede CK. Smoking behaviors of women and men in a smoking cessation clinical trial during pregnancy. Annals of Behavioral Medicine. 2008;35(Suppl 1):S199.
-
- Lasater T. [accessed 21 March 2006];Reducing ETS exposure of pregnant women and newborns. ClinicalTrials.gov. http://clinicaltrials.gov/
- Lasater TM. [accessed 21 June 2007];Tailored videos to reduce tobacco smoke exposure among pregnant women and newborns. ClinicalTrials.gov. http://clinicaltrials.gov/
Additional references
-
- Abatemarco DJ, Steinberg MB, Delnevo CD. Midwives’ knowledge, perceptions, beliefs, and practice supports regarding tobacco dependence treatment. Journal of Midwifery & Women’s Health. 2007;52:451–7. - PubMed
-
- Adams K, Melvin C. Costs of maternal conditions attributable to smoking during pregnancy. American Journal of Preventive Medicine. 1998;15(3):212–9. - PubMed
-
- Adams EK, Miller VP, Ernst C, Nishimura BK, Melvin C, Merritt R. Neonatal health care costs related to smoking during pregnancy. Health Economics. 2002;11:193–206. - PubMed
-
- Adams EK, Melvin CL, Raskind-Hood C, Joski PJ, Galactionova E. Infant delivery costs related to maternal smoking: an update. Nicotine & Tobacco Research. 2011;13:627–37. - PubMed
References to other published versions of this review
-
- Lumley J. Advice as a strategy for reducing smoking in pregnancy. [revised 02 October 1993] Pregnancy and Childbirth Module. In: Enkin MW, Keirse MJNC, Renfrew MJ, Neilson JP, Crowther C, editors. The Cochrane Pregnancy and Childbirth Database [database on disk and CDROM] The Cochrane Collaboration. Issue 2. Update Software; Oxford: 1995.
-
- Lumley J. Behavioural strategies for reducing smoking in pregnancy. [revised 27 September 1993] In: Enkin MW, Keirse MJNC, Renfrew MJ, Neilson JP, Crowther C, editors. Pregnancy and Childbirth Module. In: The Cochrane Pregnancy and Childbirth Database [database on disk and CDROM] The Cochrane Collaboration. Issue 2. Update Software; Oxford: 1995.
-
- Lumley J. Counselling for reducing smoking in pregnancy. [revised 02 October 1993] In: Enkin MW, Keirse MJNC, Renfrew MJ, Neilson JP, Crowther C, editors. Pregnancy and Childbirth Module. In: The Cochrane Pregnancy and Childbirth Database [database on disk and CDROM] The Cochrane Collaboration. Issue 2. Update Software; Oxford: 1995.
-
- Lumley J. Feedback as a strategy for reducing smoking in pregnancy. [revised 27 September 1993] Pregnancy and Childbirth Module. In: Enkin MW, Keirse MJNC, Renfrew MJ, Neilson JP, Crowther C, editors. The Cochrane Pregnancy and Childbirth Database [database on disk and CDROM] The Cochrane Collaboration. Issue 2. Update Software; Oxford: 1995.
-
- Lumley J. Strategies for reducing smoking in pregnancy. [revised 02 October 1993] Pregnancy and Childbirth Module. In: Enkin MW, Keirse MJNC, Renfrew MJ, Neilson JP, Crowther C, editors. The Cochrane Pregnancy and Childbirth Database [database on disk and CDROM] The Cochrane Collaboration. Issue 2. Update Software; Oxford: 1995.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical