

Current discharge management of acute coronary syndromes: data from the Rijnmond Collective Cardiology Research (CCR) study
- PMID: 24155103
- PMCID: PMC3890006
- DOI: 10.1007/s12471-013-0484-x
Current discharge management of acute coronary syndromes: data from the Rijnmond Collective Cardiology Research (CCR) study
Abstract
Background: Medical discharge management of acute coronary syndromes (ACS) remains suboptimal outside randomised trials and constitutes an essential quality benchmark for ACS. We sought to evaluate the rates of key guideline-recommended pharmacological agents after ACS and characteristics associated with optimal treatment at discharge.
Methods: The Rijnmond Collective Cardiology Research (CCR) registry is an ongoing prospective, observational study in the Netherlands that aims to enrol 4000 patients with ACS. We examined discharge and 1-month follow-up medication use among the first 1000 patients enrolled in the CCR registry. Logistic regression was performed to identify patient and hospital characteristics associated with collective guideline-recommended pharmacotherapy at hospital discharge.
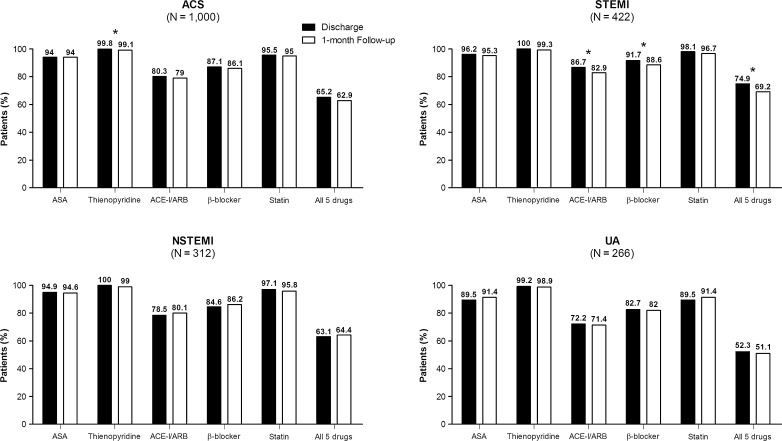
Results: At discharge, 94 % of patients received aspirin, 100 % thienopyridines, 80 % angiotensin-converting enzyme inhibitors/angiotensin-II receptor blockers, 87 % β-blockers, 96 % statins, and 65 % the combination of all 5 agents. ST-segment elevation myocardial infarction, hypertension, hypercholesterolaemia, and enrolment in an interventional centre were positive independent predictors of 5-drug combination therapy at discharge. Negative independent predictors were unstable angina and advanced age.
Conclusion: Current data from the CCR registry reflect a high quality of care for ACS discharge management in the Rotterdam-Rijnmond region. However, potential still remains for further optimisation.
Figures
References
-
- Eagle KA, Montoye CK, Riba AL, et al. Guideline-based standardized care is associated with substantially lower mortality in medicare patients with acute myocardial infarction: the American College of Cardiology’s Guidelines Applied in Practice (GAP) Projects in Michigan. J Am Coll Cardiol. 2005;46(7):1242–1248. doi: 10.1016/j.jacc.2004.12.083. - DOI - PubMed
-
- Hamm CW, Bassand JP, Agewall S, et al. ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the task force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2011;32(23):2999–3054. doi: 10.1093/eurheartj/ehr236. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
