Lymphoma affecting the breast: a pictorial review of multimodal imaging findings
- PMID: 24155754
- PMCID: PMC3800721
- DOI: 10.4048/jbc.2013.16.3.254
Lymphoma affecting the breast: a pictorial review of multimodal imaging findings
Abstract
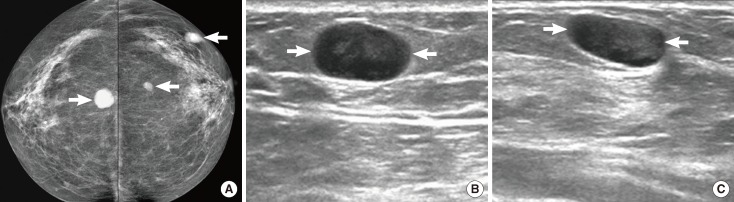
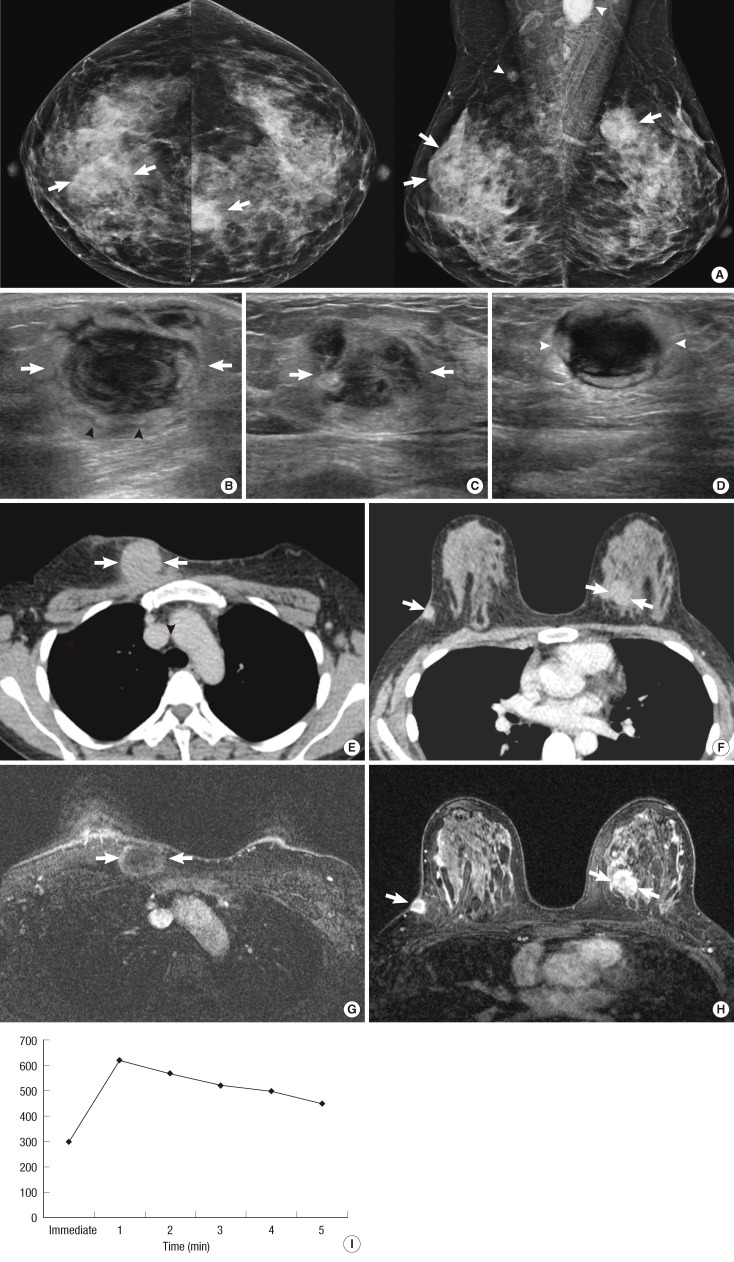
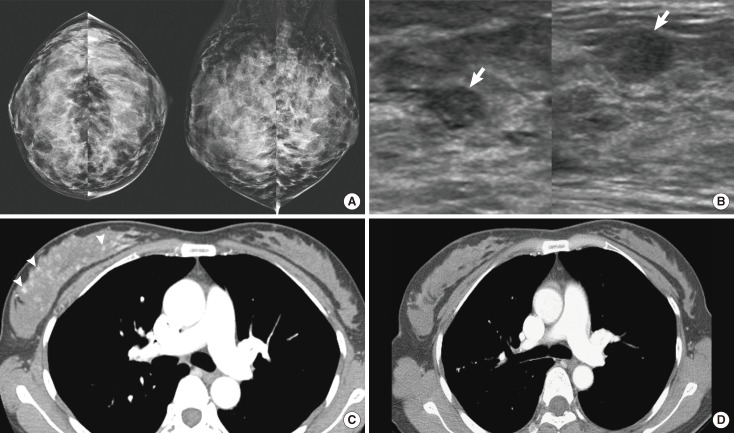
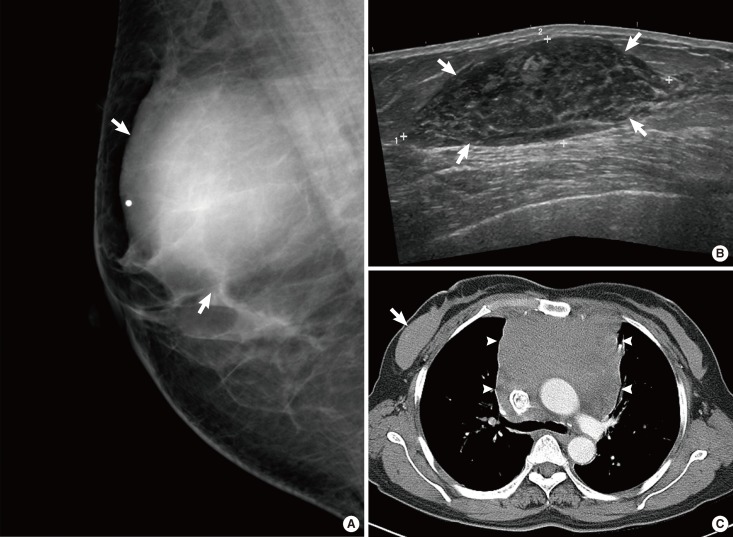
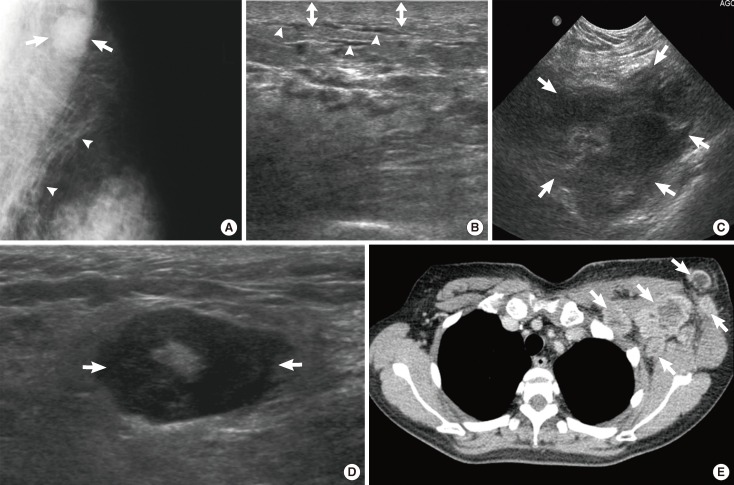
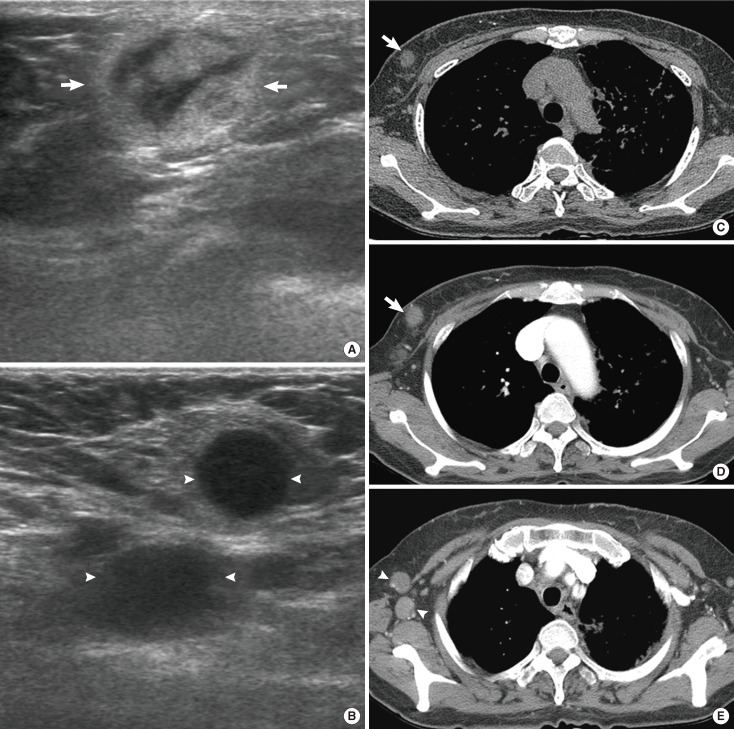
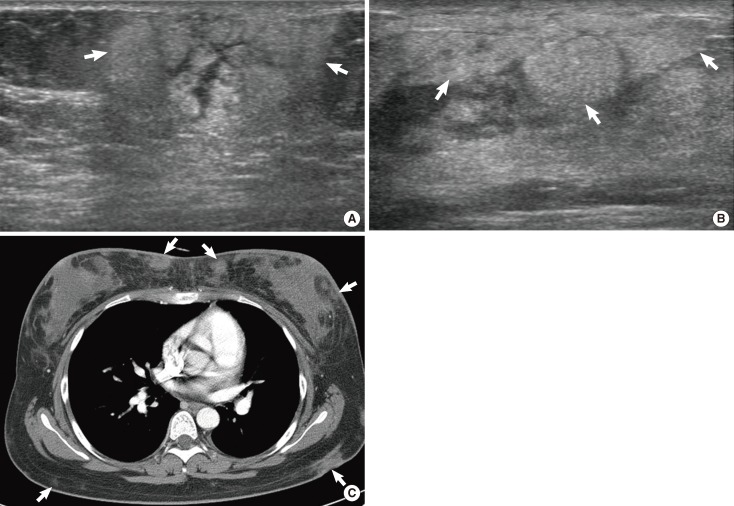
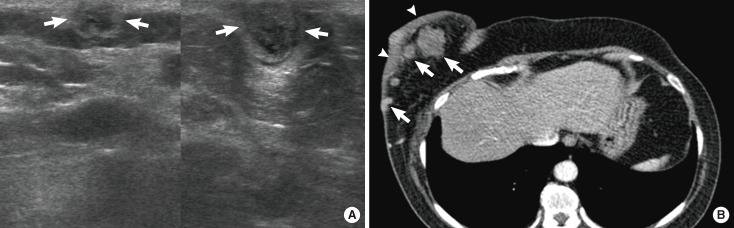
Hematological malignancies rarely affect the breast, and the majority of those that do are lymphomas. In this review, we describe the clinical aspects and multimodal imaging findings of breast lymphoma. We also illustrate the key clinical and radiological findings that allow it to be distinguished from various other malignant and benign diseases of the breast. Breast lymphoma manifests as a breast mass, a change in the subcutaneous tissue or the skin, or enlargement of the associated lymph node on radiological examination. Radiological findings associated with other breast malignancies, such as calcifications, spiculations, or architectural distortions are extremely rare. Skin and subcutaneous changes frequently accompany T-cell lymphoma. Multimodal breast imaging characteristics may aid in the diagnosis of breast lymphoma.
Keywords: Breast; Computed tomography; Lymphoma; Magnetic resonance imaging; Ultrasonography.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Swerdlow SH International Agency for Research on Cancer. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon: IARC Press; 2008.
-
- Tavassoli FA, Devilee P International Agency for Research on Cancer. Pathology and Genetics of Tumours of the Breast and Female Genital Organs. Lyon: IARC Press; 2003. pp. 9–112.
-
- Giardini R, Piccolo C, Rilke F. Primary non-Hodgkin's lymphomas of the female breast. Cancer. 1992;69:725–735. - PubMed
-
- Dao AH, Adkins RB, Jr, Glick AD. Malignant lymphoma of the breast: a review of 13 cases. Am Surg. 1992;58:792–796. - PubMed
-
- Brogi E, Harris NL. Lymphomas of the breast: pathology and clinical behavior. Semin Oncol. 1999;26:357–364. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources