

Biomarkers of lung epithelial injury and inflammation distinguish severe sepsis patients with acute respiratory distress syndrome
- PMID: 24156650
- PMCID: PMC4056313
- DOI: 10.1186/cc13080
Biomarkers of lung epithelial injury and inflammation distinguish severe sepsis patients with acute respiratory distress syndrome
Abstract
Introduction: Despite recent modifications, the clinical definition of the acute respiratory distress syndrome (ARDS) remains non-specific, leading to under-diagnosis and under-treatment. This study was designed to test the hypothesis that a biomarker panel would be useful for biologic confirmation of the clinical diagnosis of ARDS in patients at risk of developing ARDS due to severe sepsis.
Methods: This was a retrospective case control study of 100 patients with severe sepsis and no evidence of ARDS compared to 100 patients with severe sepsis and evidence of ARDS on at least two of their first four ICU days. A panel that included 11 biomarkers of inflammation, fibroblast activation, proteolytic injury, endothelial injury, and lung epithelial injury was measured in plasma from the morning of ICU day two. A backward elimination model building strategy on 1,000 bootstrapped data was used to select the best performing biomarkers for further consideration in a logistic regression model for diagnosis of ARDS.
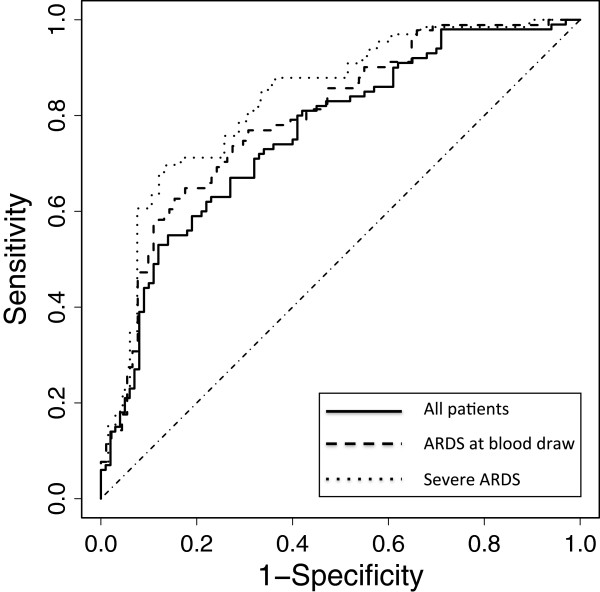
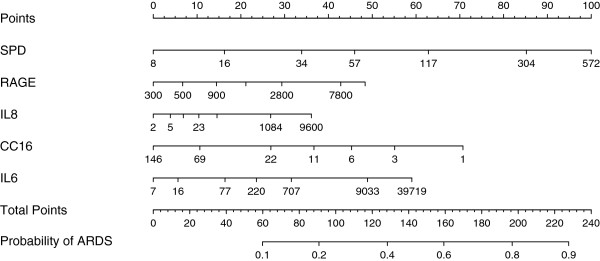
Results: Using the five best-performing biomarkers (surfactant protein-D (SP-D), receptor for advanced glycation end-products (RAGE), interleukin-8 (IL-8), club cell secretory protein (CC-16), and interleukin-6 (IL-6)) the area under the receiver operator characteristic curve (AUC) was 0.75 (95% CI: 0.7 to 0.84) for the diagnosis of ARDS. The AUC improved to 0.82 (95% CI: 0.77 to 0.90) for diagnosis of severe ARDS, defined as ARDS present on all four of the first four ICU days.
Conclusions: Abnormal levels of five plasma biomarkers including three biomarkers generated by lung epithelium (SP-D, RAGE, CC-16) provided excellent discrimination for diagnosis of ARDS in patients with severe sepsis. Altered levels of plasma biomarkers may be useful biologic confirmation of the diagnosis of ARDS in patients with sepsis, and also potentially for selecting patients for clinical trials that are designed to reduce lung epithelial injury.
Figures
Comment in
-
Rapid diagnosis of sepsis using biomarker signatures.Crit Care. 2013 Dec 4;17(6):1020. doi: 10.1186/cc13137. Crit Care. 2013. PMID: 24314350 Free PMC article.
Similar articles
-
Markers of endothelial and epithelial pulmonary injury in mechanically ventilated COVID-19 ICU patients.Crit Care. 2021 Feb 19;25(1):74. doi: 10.1186/s13054-021-03499-4. Crit Care. 2021. PMID: 33608030 Free PMC article.
-
Lung tissue expression of epithelial injury markers is associated with acute lung injury severity but does not discriminate sepsis from ARDS.Respir Res. 2024 Mar 18;25(1):129. doi: 10.1186/s12931-024-02761-x. Respir Res. 2024. PMID: 38500106 Free PMC article.
-
Plasma CC16 levels are associated with development of ALI/ARDS in patients with ventilator-associated pneumonia: a retrospective observational study.BMC Pulm Med. 2009 Dec 3;9:49. doi: 10.1186/1471-2466-9-49. BMC Pulm Med. 2009. PMID: 19958527 Free PMC article.
-
Biomarkers for the acute respiratory distress syndrome: how to make the diagnosis more precise.Ann Transl Med. 2017 Jul;5(14):283. doi: 10.21037/atm.2017.06.49. Ann Transl Med. 2017. PMID: 28828358 Free PMC article. Review.
-
A systematic review of biomarkers multivariately associated with acute respiratory distress syndrome development and mortality.Crit Care. 2020 May 24;24(1):243. doi: 10.1186/s13054-020-02913-7. Crit Care. 2020. PMID: 32448370 Free PMC article.
Cited by
-
Association of serum interleukin-6, interleukin-8, and Acute Physiology and Chronic Health Evaluation II score with clinical outcome in patients with acute respiratory distress syndrome.Indian J Crit Care Med. 2016 Sep;20(9):518-25. doi: 10.4103/0972-5229.190369. Indian J Crit Care Med. 2016. PMID: 27688627 Free PMC article.
-
Endothelial stromelysin1 regulation by the forkhead box-O transcription factors is crucial in the exudative phase of acute lung injury.Pharmacol Res. 2019 Mar;141:249-263. doi: 10.1016/j.phrs.2019.01.006. Epub 2019 Jan 3. Pharmacol Res. 2019. PMID: 30611853 Free PMC article.
-
Emerging concepts in ventilation-induced lung injury.F1000Res. 2020 Mar 31;9:F1000 Faculty Rev-222. doi: 10.12688/f1000research.20576.1. eCollection 2020. F1000Res. 2020. PMID: 32269759 Free PMC article. Review.
-
Matrix metalloproteinases and protein tyrosine kinases: potential novel targets in acute lung injury and ARDS.Chest. 2014 Oct;146(4):1081-1091. doi: 10.1378/chest.14-0397. Chest. 2014. PMID: 25287998 Free PMC article. Review.
-
Preventing ARDS: progress, promise, and pitfalls.Chest. 2014 Oct;146(4):1102-1113. doi: 10.1378/chest.14-0555. Chest. 2014. PMID: 25288000 Free PMC article.
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, Camporota L, Slutsky AS. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;17:2526–2533. - PubMed
-
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, Legall JR, Morris A, Spragg R. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;17:818–824. doi: 10.1164/ajrccm.149.3.7509706. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
