

Continued improvement in survival in multiple myeloma: changes in early mortality and outcomes in older patients
- PMID: 24157580
- PMCID: PMC4000285
- DOI: 10.1038/leu.2013.313
Continued improvement in survival in multiple myeloma: changes in early mortality and outcomes in older patients
Abstract
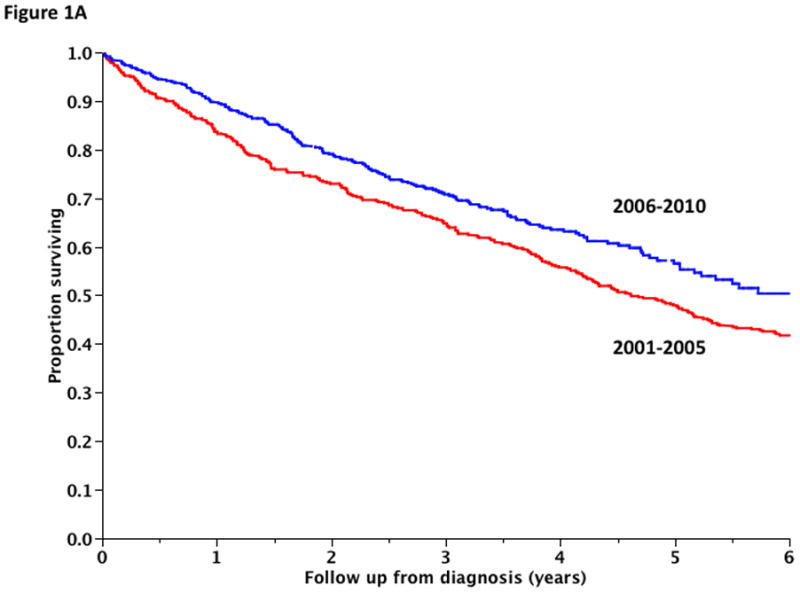
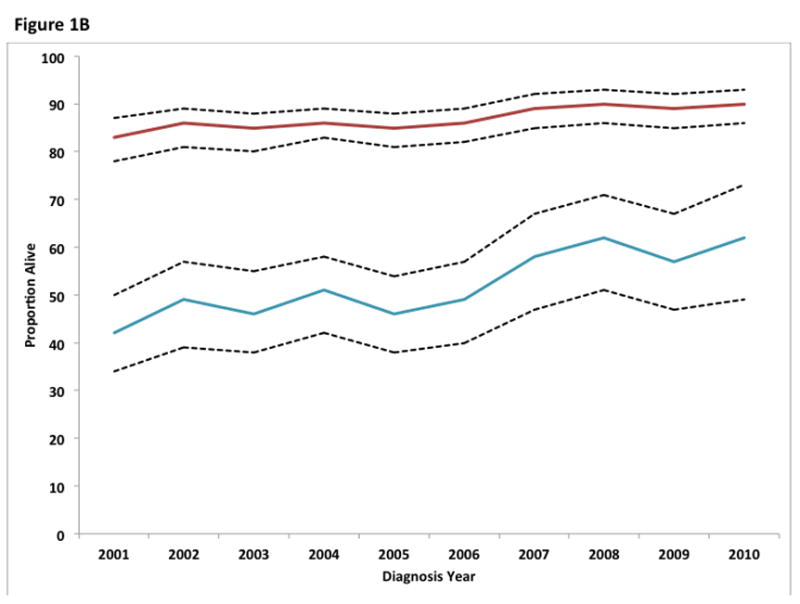
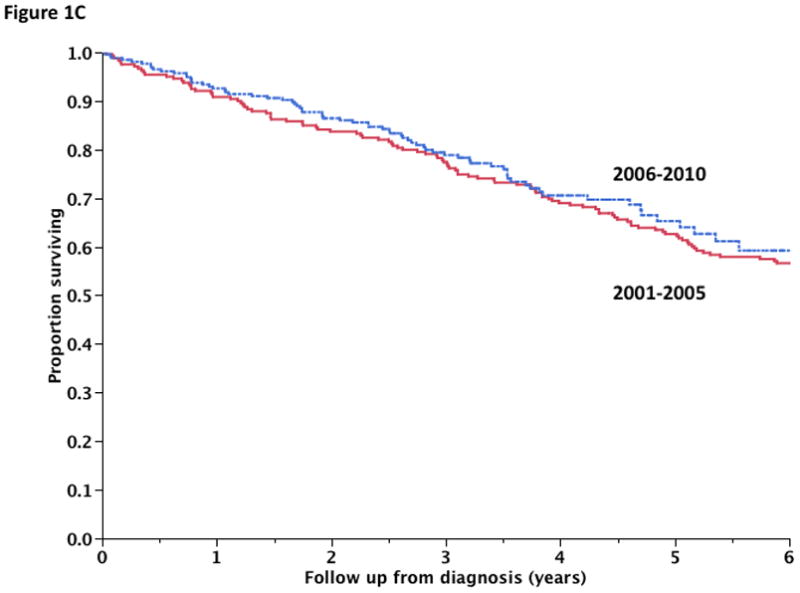
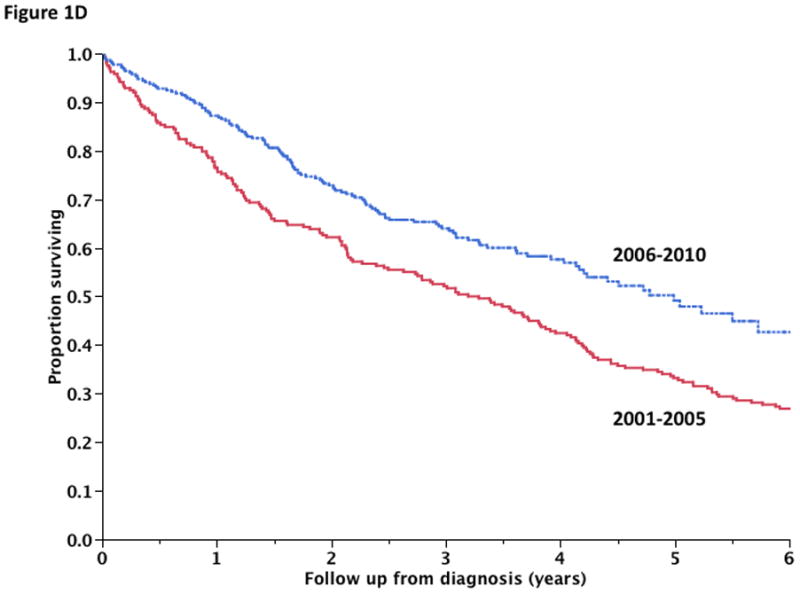
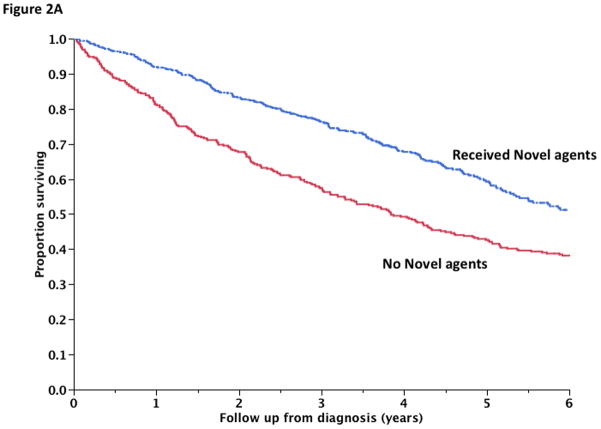
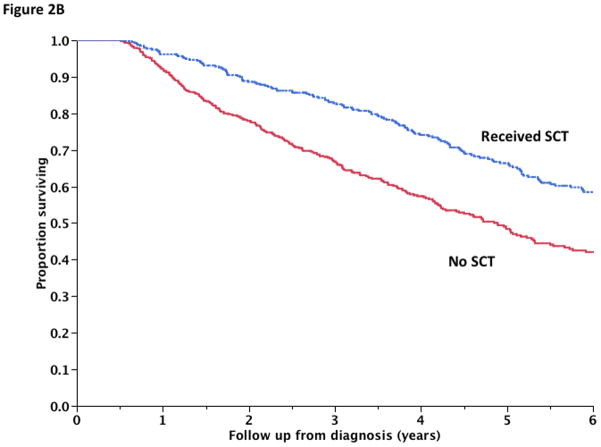
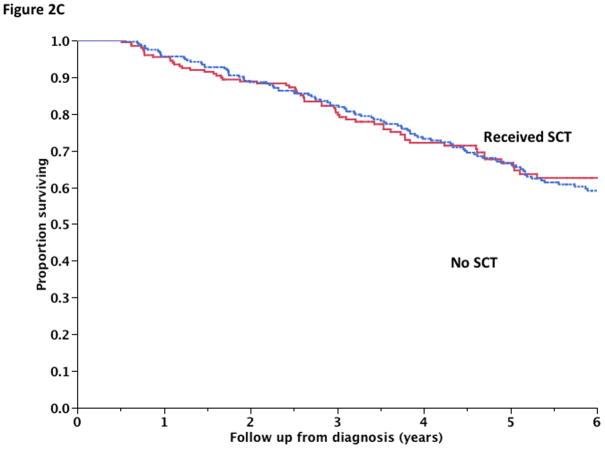
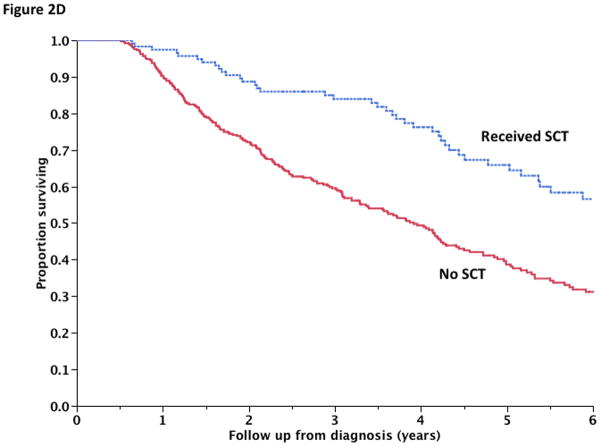
Therapy for multiple myeloma (MM) has markedly changed in the past decade with the introduction of new drugs, but it is not clear whether the improvements have been sustained. We studied 1038 patients diagnosed between 2001 and 2010, grouping patients into two 5-year periods by diagnosis, 2001-2005 and 2006-2010. The median estimated follow-up for the cohort was 5.9 years with 47% alive at the last follow-up. The median overall survival (OS) for the entire cohort was 5.2 years: 4.6 years for patients in the 2001-2005 group compared with 6.1 years for the 2006-2010 cohort (P=0.002). The improvement was primarily seen among patients over 65 years, the 6-year OS improving from 31 to 56%, P<0.001. Only 10% of patients died during the first year in the latter group, compared with 16% in the earlier cohort (P<0.01), suggesting improvement in early mortality. The improved outcomes were linked closely to the use of one or more new agents in initial therapy. The current results confirm continued survival improvement in MM and highlight the impact of initial therapy with novel agents. Most importantly, we demonstrate that the improved survival is benefitting older patients and that early mortality in this disease has reduced considerably.
Figures

References
-
- Mikhael JR, Dingli D, Roy V, Reeder CB, Buadi FK, Hayman SR, et al. Management of Newly Diagnosed Symptomatic Multiple Myeloma: Updated Mayo Stratification of Myeloma and Risk-Adapted Therapy (mSMART) Consensus Guidelines 2013. Mayo Clin Proc. 2013 Apr;88(4):360–376. - PubMed
-
- Kyle RA. Targeted therapy of multiple myeloma. Hematology. 2012 Apr;17(Suppl 1):S125–128. - PubMed
-
- Brenner H, Gondos A, Pulte D. Recent major improvement in long-term survival of younger patients with multiple myeloma. Blood. 2008 Mar 1;111(5):2521–2526. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
