

Cardiovascular health knowledge, attitude and practice/behaviour in an urbanising community of Nepal: a population-based cross-sectional study from Jhaukhel-Duwakot Health Demographic Surveillance Site
- PMID: 24157816
- PMCID: PMC3808775
- DOI: 10.1136/bmjopen-2013-002976
Cardiovascular health knowledge, attitude and practice/behaviour in an urbanising community of Nepal: a population-based cross-sectional study from Jhaukhel-Duwakot Health Demographic Surveillance Site
Abstract
Objectives: This study determined the knowledge, attitude and practice/behaviour of cardiovascular health in residents of a semiurban community of Nepal.
Design: To increase the understanding of knowledge, attitude and practice/behaviour towards cardiovascular health, we conducted in-home interviews using a questionnaire based on the WHO STEPwise approach to surveillance and other resources, scoring all responses. We also recorded blood pressure and took anthropometric measurements.
Setting: Our study was conducted as part of the Heart-Health-Associated Research and Dissemination in the Community project in the Jhaukhel-Duwakot Health Demographic Surveillance Site in two urbanising villages near Kathmandu.
Participants: The study population included 777 respondents from six randomly selected clusters in both villages.
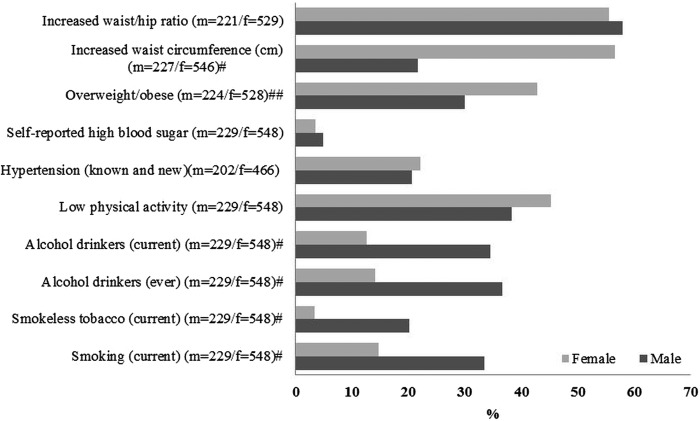
Results: Seventy per cent of all participants were women and 26.9% lacked formal education. The burden of cardiovascular risk factors was high; 20.1% were current smokers, 43.3% exhibited low physical activity and 21.6% were hypertensive. Participants showed only poor knowledge of heart disease causes; 29.7% identified hypertension and 11% identified overweight and physical activity as causes, whereas only 2.2% identified high blood sugar as causative. Around 60% of respondents did not know any heart attack symptoms compared with 20% who knew 2-4 symptoms. Median percentage scores for knowledge, attitude and practice/behaviour were 79.3, 74.3 and 48, respectively. Nearly 44% of respondents had insufficient knowledge and less than 20% had highly satisfactory knowledge. Among those with highly satisfactory knowledge, only 14.7% had a highly satisfactory attitude and 19.5% and 13.9% had satisfactory and highly satisfactory practices, respectively.
Conclusions: Our study demonstrates a gap between cardiovascular health knowledge, attitude and practice/behaviour in a semiurban community in a low-income nation, even among those already affected by cardiovascular disease.
Keywords: Epidemiology; Preventive Medicine; Public Health.
Figures
Similar articles
-
Knowledge, attitude and practice on diet and physical activity among mothers with young children in the Jhaukhel-Duwakot Health Demographic Surveillance Site, Nepal.PLoS One. 2018 Jul 9;13(7):e0200329. doi: 10.1371/journal.pone.0200329. eCollection 2018. PLoS One. 2018. PMID: 29985946 Free PMC article.
-
Understanding and living with glaucoma and non-communicable diseases like hypertension and diabetes in the Jhaukhel-Duwakot Health Demographic Surveillance Site: a qualitative study from Nepal.Glob Health Action. 2014 Oct 20;7:25358. doi: 10.3402/gha.v7.25358. eCollection 2014. Glob Health Action. 2014. PMID: 25361727 Free PMC article.
-
Physical activity level and its sociodemographic correlates in a peri-urban Nepalese population: a cross-sectional study from the Jhaukhel-Duwakot health demographic surveillance site.Int J Behav Nutr Phys Act. 2014 Mar 14;11(1):39. doi: 10.1186/1479-5868-11-39. Int J Behav Nutr Phys Act. 2014. PMID: 24628997 Free PMC article.
-
Correlates of smoking susceptibility among adolescents in a peri-urban area of Nepal: a population-based cross-sectional study in the Jhaukhel-Duwakot Health Demographic Surveillance Site.Glob Health Action. 2014 Jul 16;7:24488. doi: 10.3402/gha.v7.24488. eCollection 2014. Glob Health Action. 2014. PMID: 25034345 Free PMC article.
-
Uterine prolapse and its impact on quality of life in the Jhaukhel-Duwakot Health Demographic Surveillance Site, Bhaktapur, Nepal.Glob Health Action. 2015 Aug 10;8:28771. doi: 10.3402/gha.v8.28771. eCollection 2015. Glob Health Action. 2015. PMID: 26265389 Free PMC article.
Cited by
-
Knowledge, attitudes, and preventative practices regarding ischemic heart disease among emergency department patients in northern Tanzania.Public Health. 2019 Oct;175:60-67. doi: 10.1016/j.puhe.2019.06.017. Epub 2019 Aug 8. Public Health. 2019. PMID: 31401252 Free PMC article.
-
Sharing the power through promoting heart health literacy: A participatory action research in Iran.ARYA Atheroscler. 2019 May;15(3):146-151. doi: 10.22122/arya.v15i3.1902. ARYA Atheroscler. 2019. PMID: 31452663 Free PMC article.
-
Knowledge, Attitude, and Practice Regarding Cardiovascular Diseases in Adults Attending Health Care Centers in Tehran, Iran.Int J Endocrinol Metab. 2020 Oct 1;18(3):e101612. doi: 10.5812/ijem.101612. eCollection 2020 Jul. Int J Endocrinol Metab. 2020. PMID: 33257905 Free PMC article.
-
Knowledge, Attitude, and Behaviors Related to Eating Out among University Students in China.Int J Environ Res Public Health. 2016 Jul 12;13(7):696. doi: 10.3390/ijerph13070696. Int J Environ Res Public Health. 2016. PMID: 27420075 Free PMC article.
-
Illness perception and cardiovascular health behaviour among persons with ischemic heart disease in Indonesia.Int J Nurs Sci. 2018 Apr 16;5(2):174-180. doi: 10.1016/j.ijnss.2018.04.007. eCollection 2018 Apr 10. Int J Nurs Sci. 2018. PMID: 31406821 Free PMC article.
References
-
- Alwan A. Global status report on noncommunicable diseases 2010. Geneva: World Health Organization, 2011
-
- World Health Organization Noncommunicable diseases in the South-East Asia Region: situation and response 2011. New Delhi: World Health Organization, Regional Office for South-East Asia, 2011
-
- Reddy KS. Cardiovascular diseases in the developing countries: dimensions, determinants, dynamics and directions for public health action. Public Health Nutr 2002;5:231–7 - PubMed
-
- Reddy KS, Yusuf S. Emerging epidemic of cardiovascular disease in developing countries. Circulation 1998;97:596–601 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous