

Mining clinical text for signals of adverse drug-drug interactions
- PMID: 24158091
- PMCID: PMC3932451
- DOI: 10.1136/amiajnl-2013-001612
Mining clinical text for signals of adverse drug-drug interactions
Abstract
Background and objective: Electronic health records (EHRs) are increasingly being used to complement the FDA Adverse Event Reporting System (FAERS) and to enable active pharmacovigilance. Over 30% of all adverse drug reactions are caused by drug-drug interactions (DDIs) and result in significant morbidity every year, making their early identification vital. We present an approach for identifying DDI signals directly from the textual portion of EHRs.
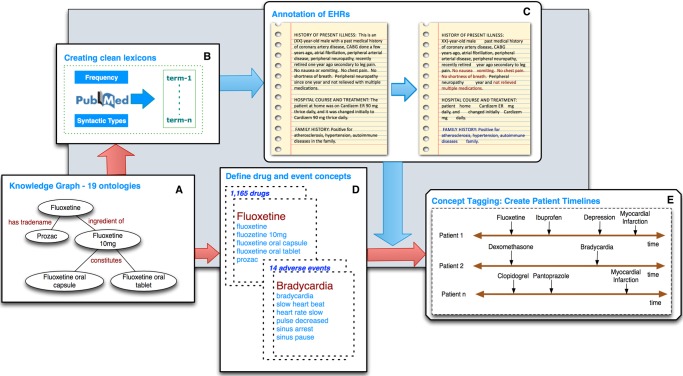
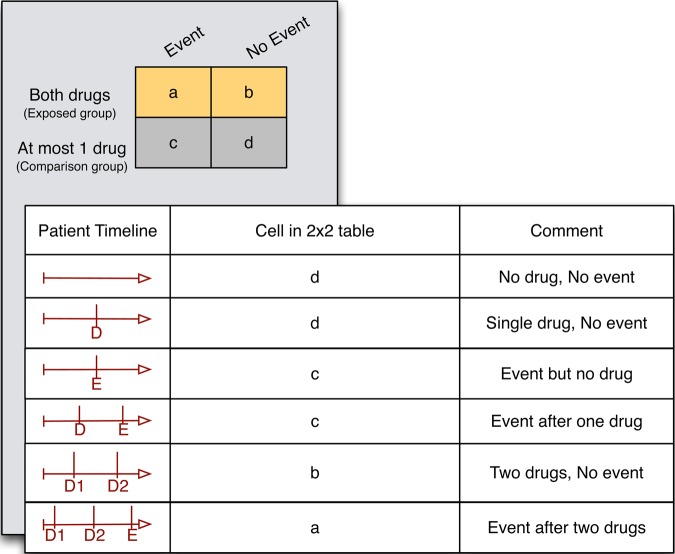
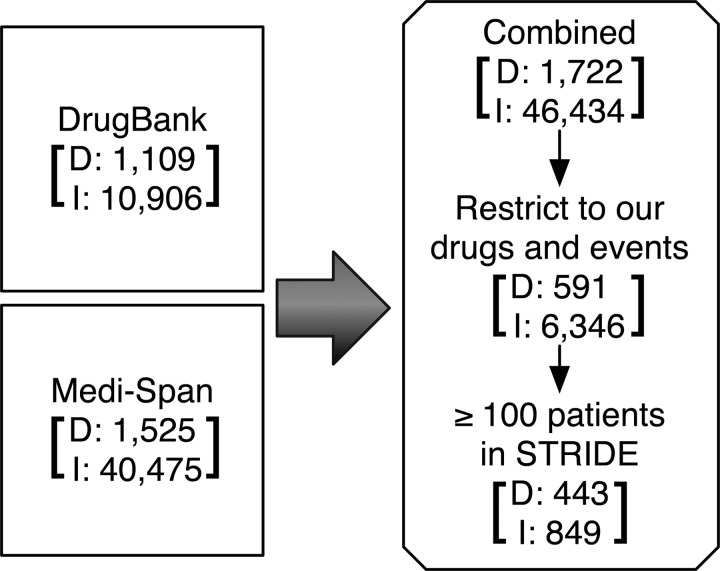
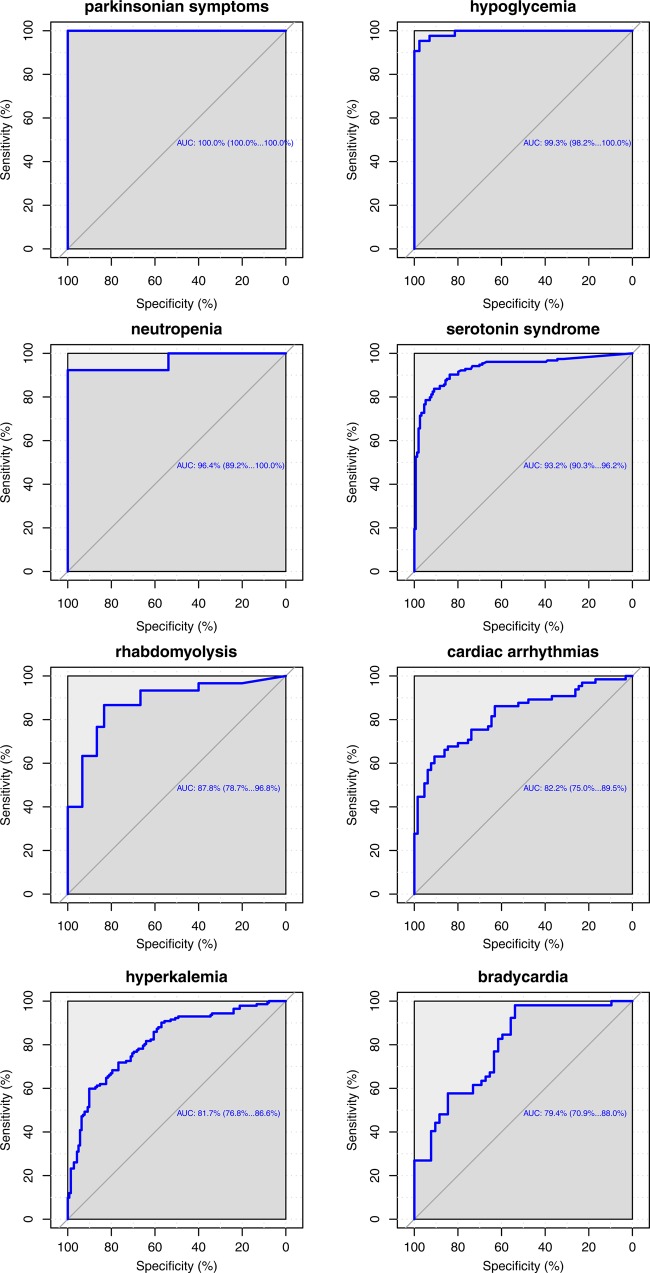
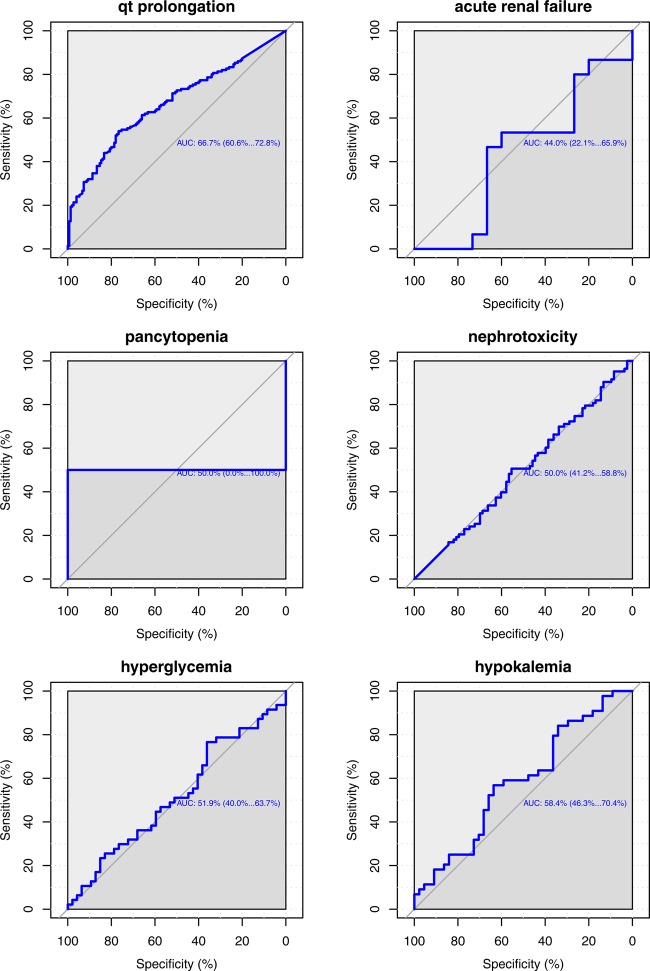
Methods: We recognize mentions of drug and event concepts from over 50 million clinical notes from two sites to create a timeline of concept mentions for each patient. We then use adjusted disproportionality ratios to identify significant drug-drug-event associations among 1165 drugs and 14 adverse events. To validate our results, we evaluate our performance on a gold standard of 1698 DDIs curated from existing knowledge bases, as well as with signaling DDI associations directly from FAERS using established methods.
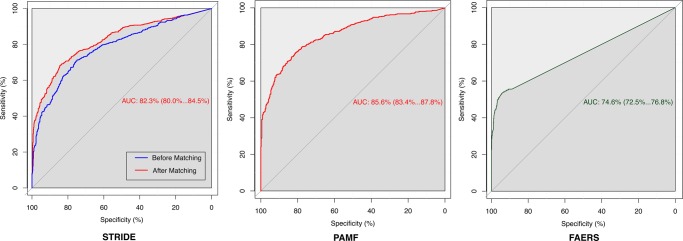
Results: Our method achieves good performance, as measured by our gold standard (area under the receiver operator characteristic (ROC) curve >80%), on two independent EHR datasets and the performance is comparable to that of signaling DDIs from FAERS. We demonstrate the utility of our method for early detection of DDIs and for identifying alternatives for risky drug combinations. Finally, we publish a first of its kind database of population event rates among patients on drug combinations based on an EHR corpus.
Conclusions: It is feasible to identify DDI signals and estimate the rate of adverse events among patients on drug combinations, directly from clinical text; this could have utility in prioritizing drug interaction surveillance as well as in clinical decision support.
Keywords: Adverse Reactions; Data Mining; Drug Interaction; Electronic Health Records; Ontology; Pharmacovigilance.
Figures
References
-
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA 1998;279:1200–5 - PubMed
-
- Johnson JA, Bootman JL. Drug-related morbidity and mortality. A cost-of-illness model. Arch Intern Med 1995;155:1949–56 - PubMed
-
- Pirohamed M. Drug interactions of clinical importance. London: Chapman and Hall, 1998
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
