

The cost-effectiveness of deep brain stimulation in combination with best medical therapy, versus best medical therapy alone, in advanced Parkinson's disease
- PMID: 24158271
- PMCID: PMC3895185
- DOI: 10.1007/s00415-013-7148-z
The cost-effectiveness of deep brain stimulation in combination with best medical therapy, versus best medical therapy alone, in advanced Parkinson's disease
Abstract
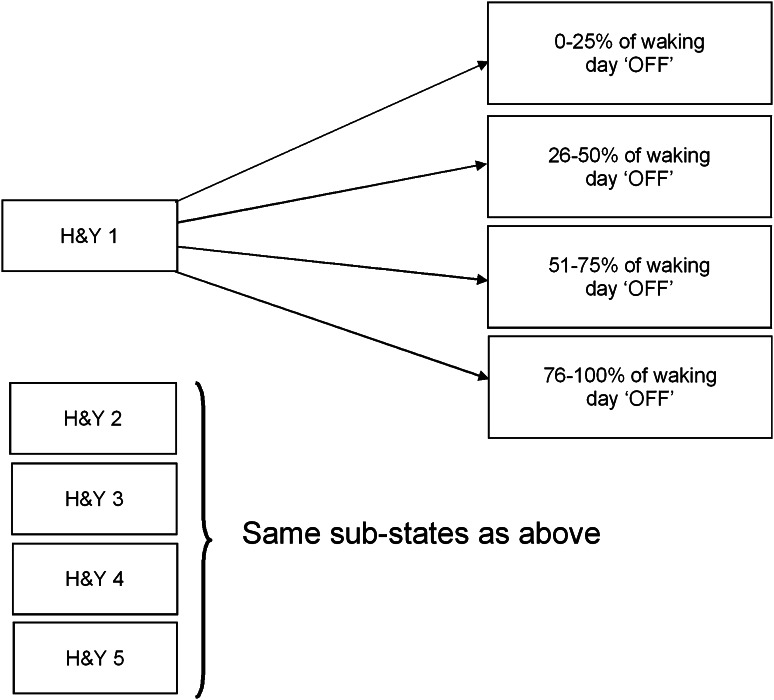
Parkinson's disease (PD) is a complex progressive movement disorder leading to motor and non-motor symptoms that become increasingly debilitating as the disease advances, considerably reducing quality of life. Advanced treatment options include deep brain stimulation (DBS). While clinical effectiveness of DBS has been demonstrated in a number of randomised controlled trials (RCT), evidence on cost-effectiveness is limited. The cost-effectiveness of DBS combined with BMT, versus BMT alone, was evaluated from a UK payer perspective. Individual patient-level data on the effect of DBS on PD symptom progression from a large 6-month RCT were used to develop a Markov model representing clinical progression and capture treatment effect and costs. A 5-year time horizon was used, and an incremental cost-effectiveness ratio (ICER) was calculated in terms of cost per quality-adjusted life-years (QALY) and uncertainty assessed in deterministic sensitivity analyses. Total discounted costs in the DBS and BMT groups over 5 years were £68,970 and £48,243, respectively, with QALYs of 2.21 and 1.21, giving an incremental cost-effectiveness ratio of £20,678 per QALY gained. Utility weights in each health state and costs of on-going medication appear to be the key drivers of uncertainty in the model. The results suggest that DBS is a cost-effective intervention in patients with advanced PD who are eligible for surgery, providing good value for money to health care payers.
Figures



References
-
- Wickremaratchi MM, Perera D, O’Loghlen C, Sastry D, Morgan E, Jones A, Edwards P, Robertson NP, Butler C, Morris HR, Ben-Shlomo Y. Prevalence and age of onset of Parkinson’s disease in Cardiff: a community based cross sectional study and meta-analysis. J Neurol Neurosurg Psychiatry. 2008;80(7):805–807. doi: 10.1136/jnnp.2008.162222. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
