

A century of optocardiography
- PMID: 24158521
- PMCID: PMC4521770
- DOI: 10.1109/RBME.2013.2286296
A century of optocardiography
Abstract
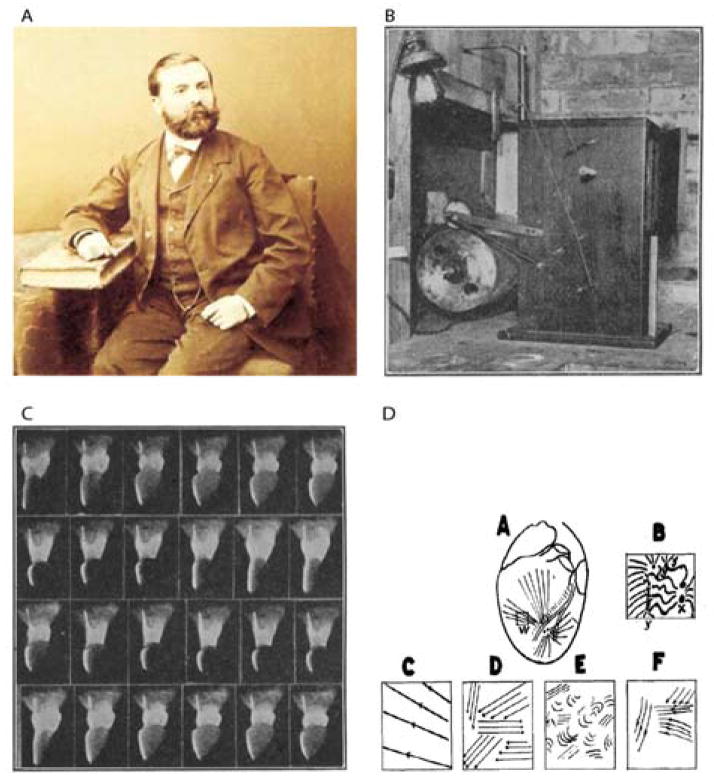
In the past decade, optical mapping provided crucial mechanistic insight into electromechanical function and the mechanism of ventricular fibrillation. Therefore, to date, optical mapping dominates experimental cardiac electrophysiology. The first cardiac measurements involving optics were done in the early 1900s using the fast cinematograph that later evolved into methods for high-resolution activation and repolarization mapping and stimulation of specific cardiac cell types. The field of "optocardiography," therefore, emerged as the use of light for recording or interfering with cardiac physiology. In this review, we discuss how optocardiography developed into the dominant research technique in experimental cardiology. Furthermore, we envision how optocardiographic methods can be used in clinical cardiology.
Figures
References
-
- Koelliker RAMH. Nachweis der negativen Schwankung des Muskelstroms am naturlich sich contrahirenden Muskel. Verhandlungen der Physikalisch-medizinische Gesellschaft in Würzburg. 1856;6:15.
-
- Oster HS, Taccardi B, Lux RL, Ershler PR, Rudy Y. Noninvasive electrocardiographic imaging: reconstruction of epicardial potentials, electrograms, and isochrones and localization of single and multiple electrocardiac events. Circulation. 1997 Aug 5;96:1012–24. - PubMed
-
- Lewalter TLB. Historical Milestones of Electrical Signal Recording and Analysis. In: Gussak IAC, editor. Briding Basic and Clinical Science. New Jersey: Humana Press Inc; 2010. pp. 7–21.
-
- Efimov IR, Nikolski VP, Salama G. Optical imaging of the heart. Circulation Research. 2004;95:21–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
