

Country- and age-specific optimal allocation of dengue vaccines
- PMID: 24161462
- PMCID: PMC3947060
- DOI: 10.1016/j.jtbi.2013.10.006
Country- and age-specific optimal allocation of dengue vaccines
Abstract
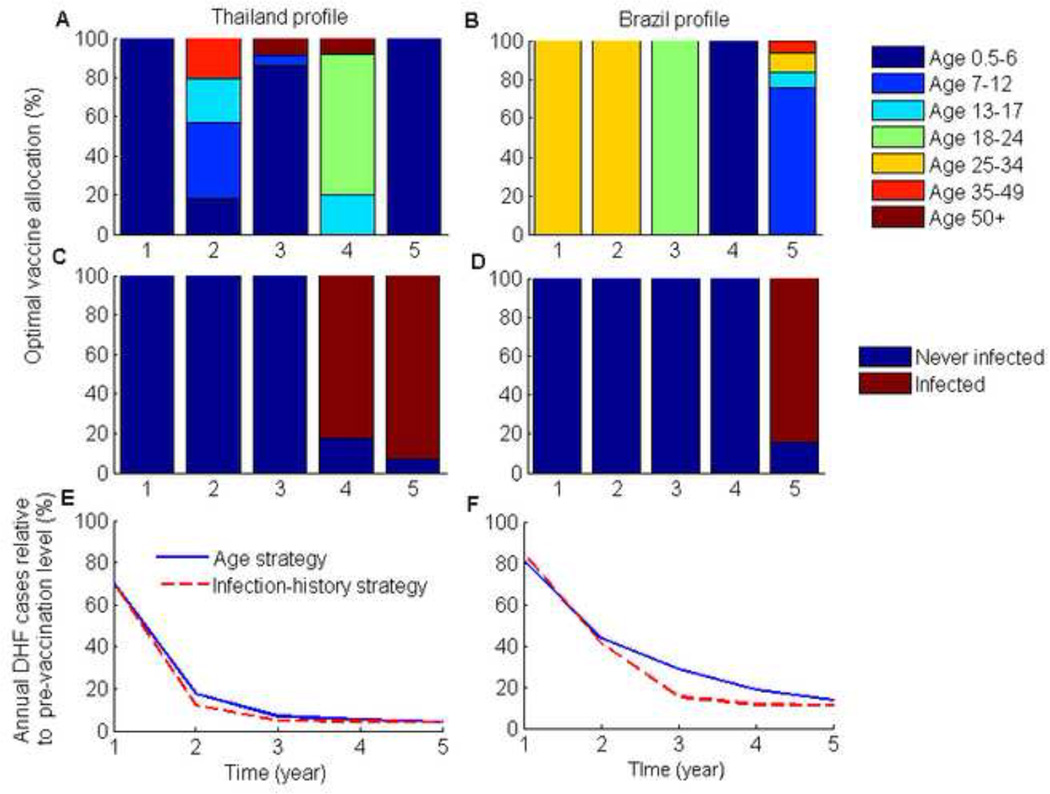
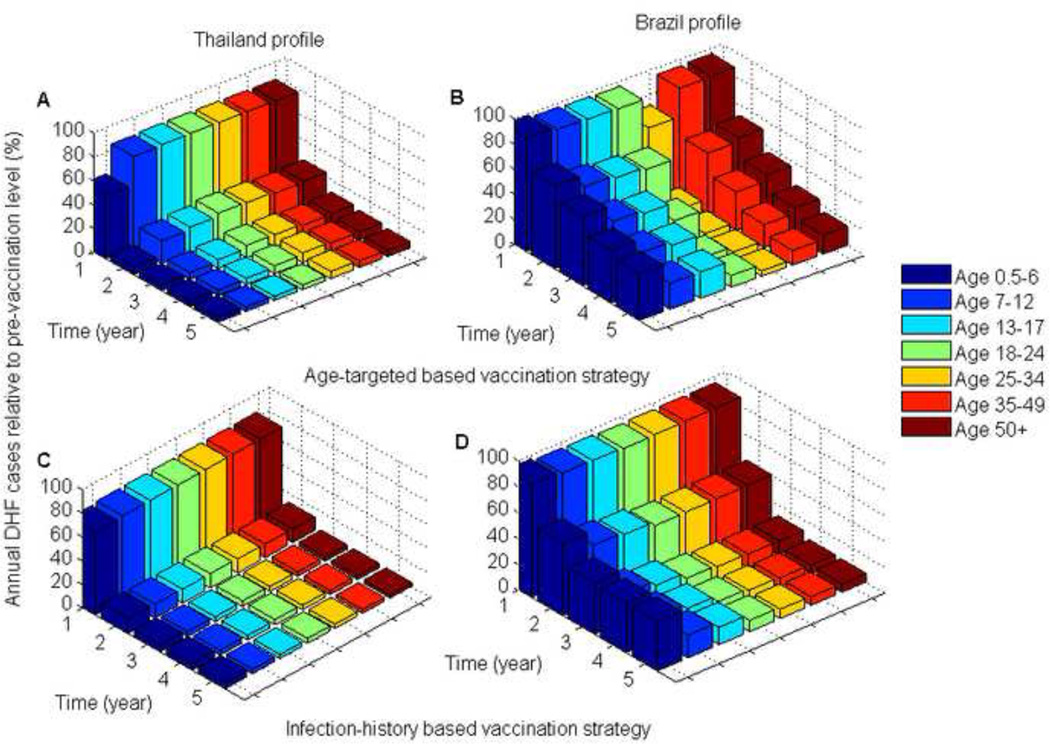
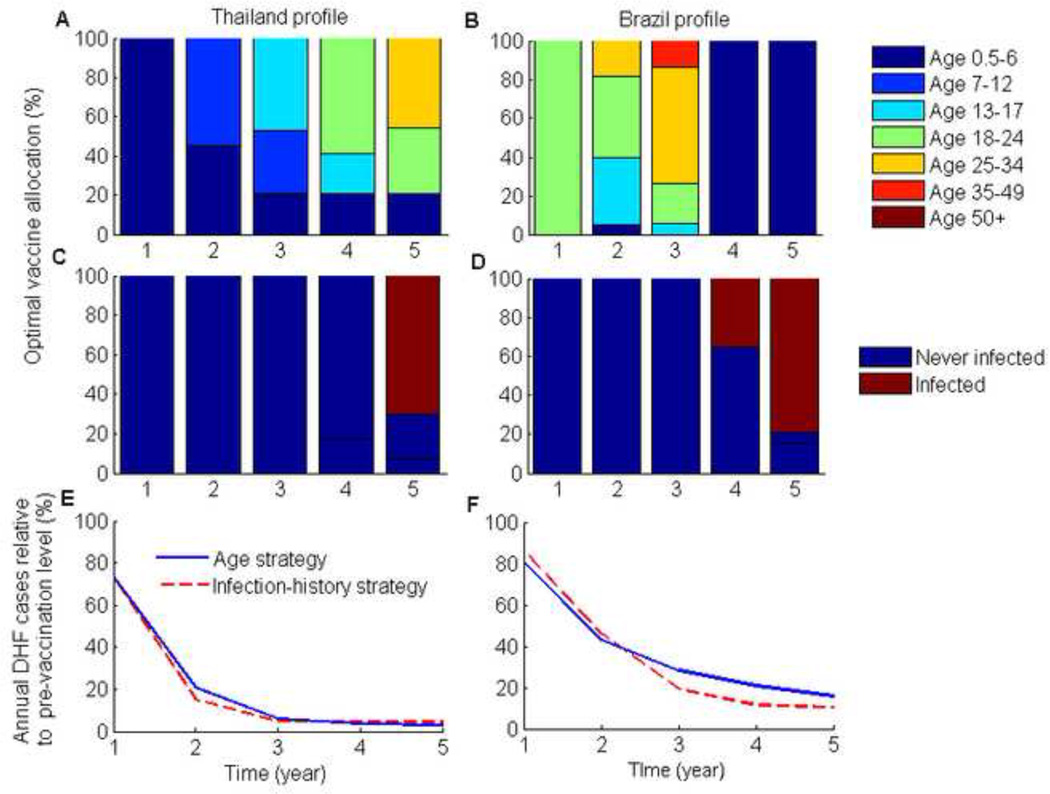
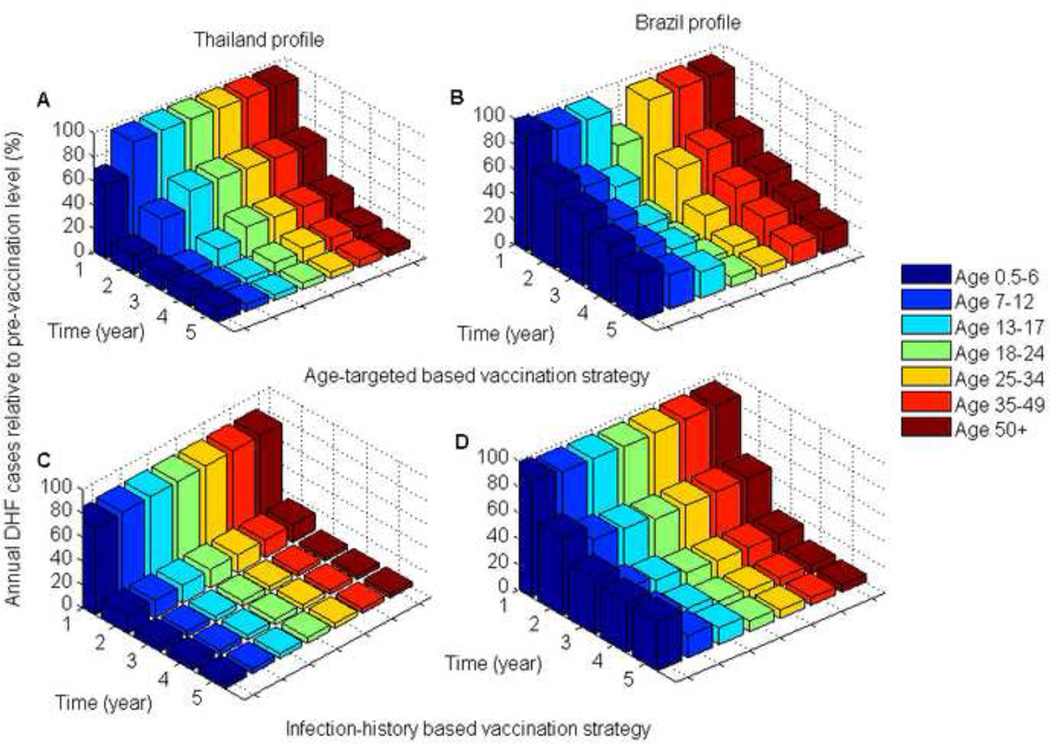
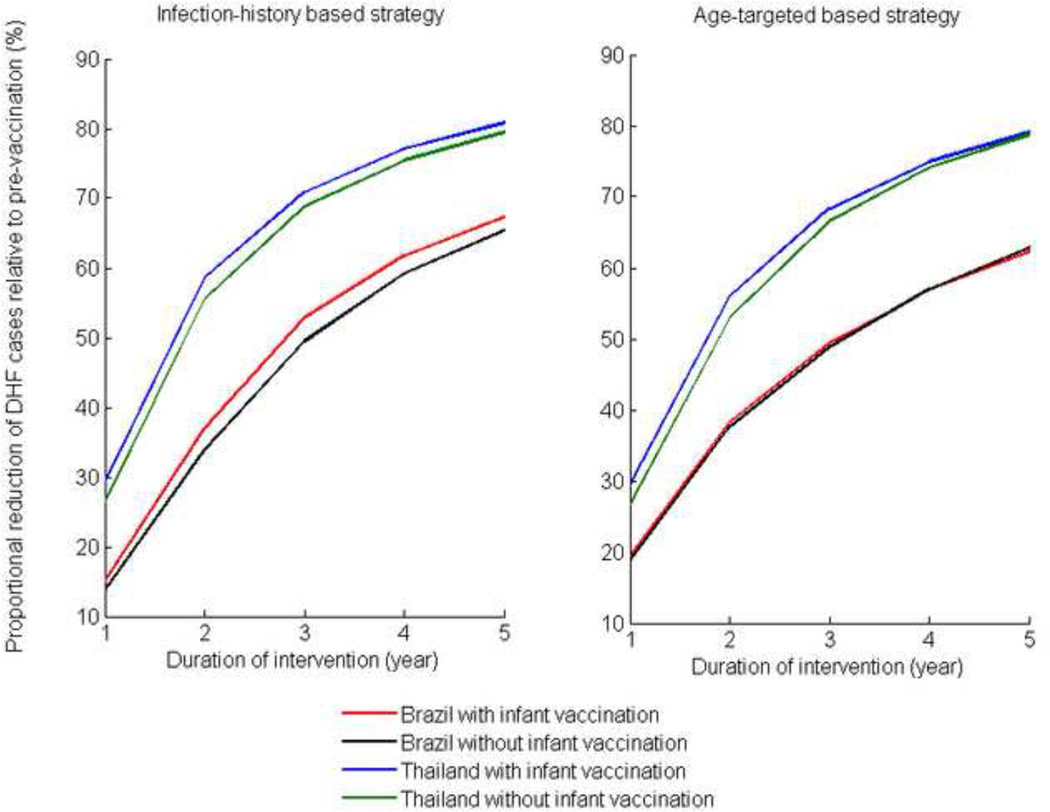
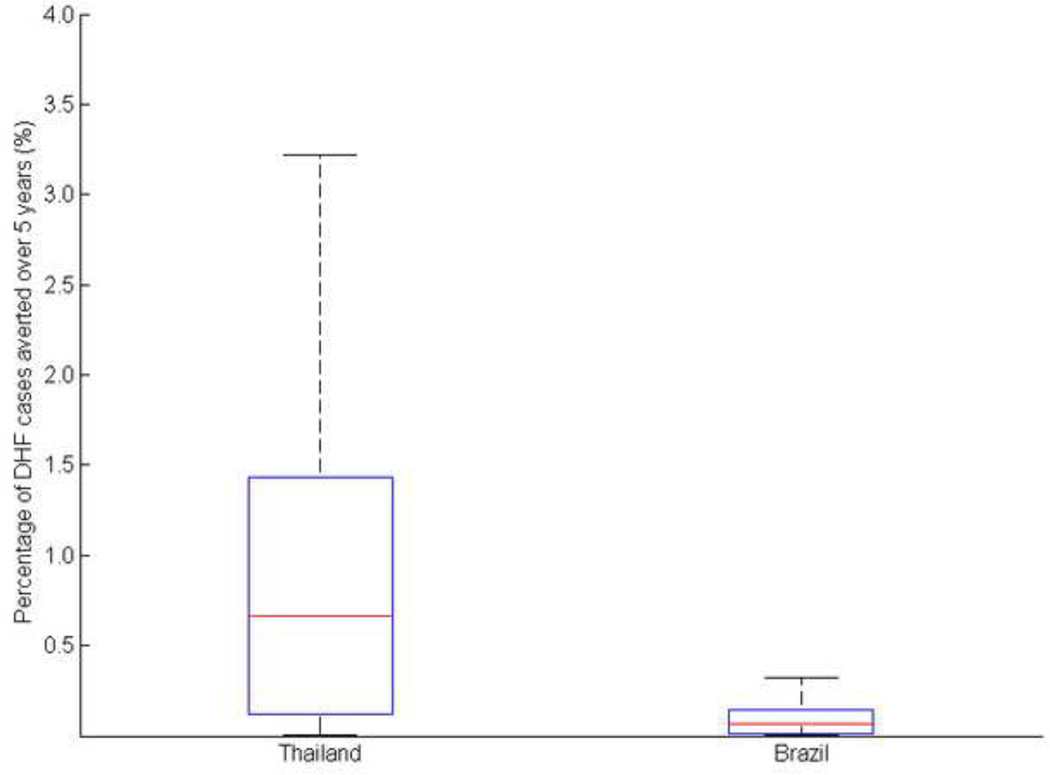
Several dengue vaccines are under development, and some are expected to become available imminently. Concomitant with the anticipated release of these vaccines, vaccine allocation strategies for dengue-endemic countries in Southeast Asia and Latin America are currently under development. We developed a model of dengue transmission that incorporates the age-specific distributions of dengue burden corresponding to those in Thailand and Brazil, respectively, to determine vaccine allocations that minimize the incidence of dengue hemorrhagic fever, taking into account limited availability of vaccine doses in the initial phase of production. We showed that optimal vaccine allocation strategies vary significantly with the demographic burden of dengue hemorrhagic fever. Consequently, the strategy that is optimal for one country may be sub-optimal for another country. More specifically, we showed that, during the first years following introduction of a dengue vaccine, it is optimal to target children for dengue mass vaccination in Thailand, whereas young adults should be targeted in Brazil.
Keywords: Dengue hemorrhagic fever; Dengue vaccine; Mathematical modeling; Optimization.
© 2013 Published by Elsevier Ltd.
Figures
References
-
- Suaya JA, Shepard DS, Siqueira JB, Martelli CT, Lum LCS, Tan LH, et al. Cost of dengue cases in eight countries in the Americas and Asia: a prospective study. The American journal of tropical medicine and hygiene. 2009;80(5):846–855. - PubMed
-
- Halstead SB. Dengue. The Lancet. 2007;370(9599):1644–1652. - PubMed
-
- Murrell S, Wu SC, Butler M. Review of dengue virus and the development of a vaccine. Biotechnology advances. 2011;29(2):239–247. - PubMed
-
- Srikiatkhachorn A, Gibbons RV, Green S, Libraty DH, Thomas SJ, Endy TP, et al. Dengue Hemorrhagic Fever: The Sensitivity and Specificity of the World Health Organization Definition for Identification of Severe Cases of Dengue in Thailand, 1994–2005. Clinical Infectious Diseases. 2010 Apr 15;50(8):1135–1143. 2010. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
