

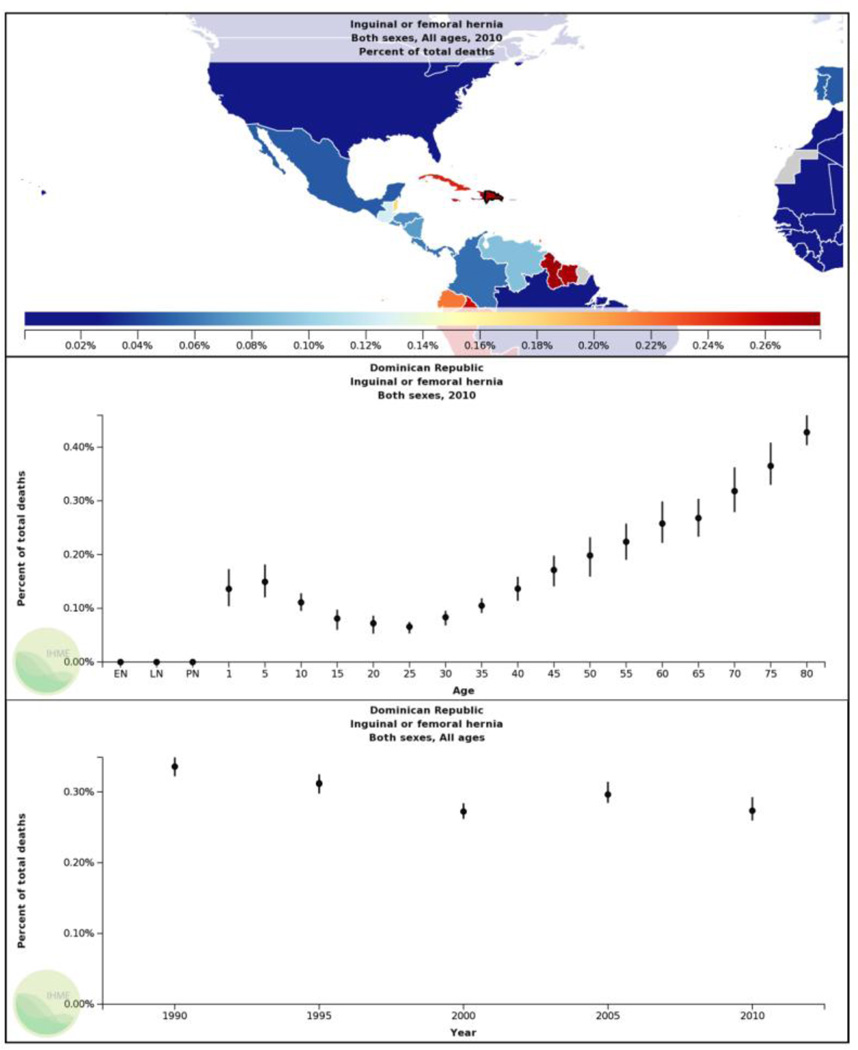
A material cost-minimization analysis for hernia repairs and minor procedures during a surgical mission in the Dominican Republic
- PMID: 24162140
- PMCID: PMC3943836
- DOI: 10.1007/s00464-013-3253-4
A material cost-minimization analysis for hernia repairs and minor procedures during a surgical mission in the Dominican Republic
Abstract
Introduction: Expenditures on material supplies and medications constitute the greatest per capita costs for surgical missions. We hypothesized that supply acquisition at non-profit organization (NPO) costs would lead to significant cost-savings compared with supply acquisition at US academic institution costs from the provider perspective for hernia repairs and minor procedures during a surgical mission in the Dominican Republic.
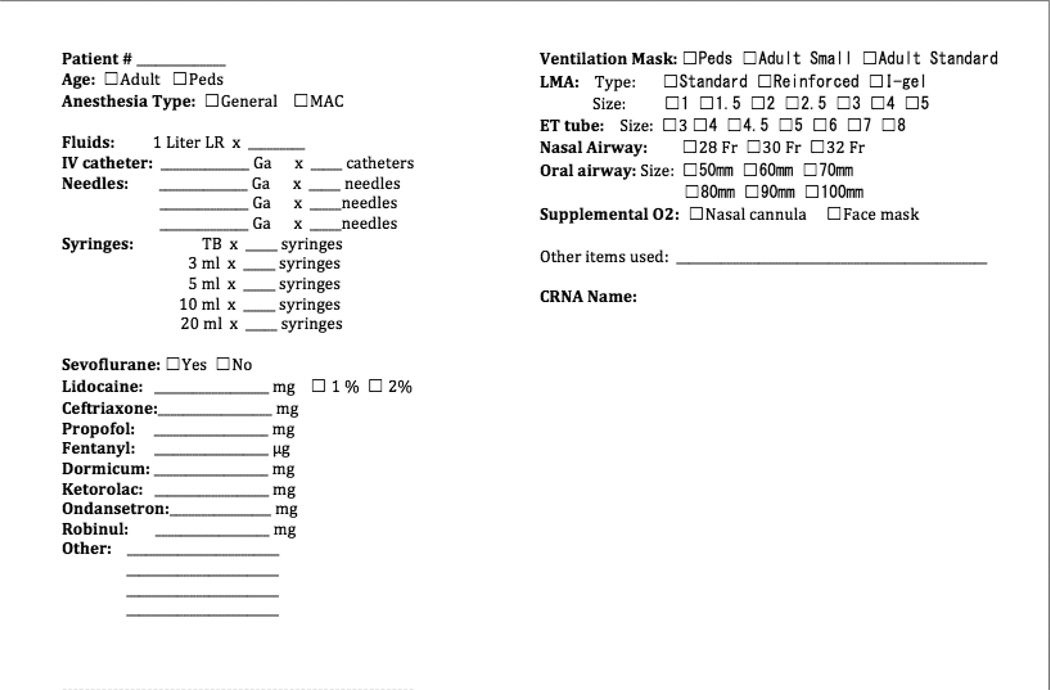
Methods: Items acquired for a surgical mission were uniquely QR-coded for accurate consumption accounting. Both NPO and US academic institution unit costs were associated with each item in an electronic inventory system. Medication doses were recorded and QR codes for consumed items were scanned into a record for each sampled procedure. Mean material costs and cost-savings ± SDs were calculated in US dollars for each procedure type. Cost-minimization analyses between the NPO and the US academic institution platforms for each procedure type ensued using a two-tailed Wilcoxon matched-pairs test with α = 0.05. Item utilization analyses generated lists of most frequently used materials by procedure type.
Results: The mean cost-savings of supply acquisition at NPO costs for each procedure type were as follows: $482.86 ± $683.79 for unilateral inguinal hernia repair (n = 13); $332.46 ± $184.09 for bilateral inguinal hernia repair (n = 3); $127.26 ± $13.18 for hydrocelectomy (n = 9); $232.92 ± $56.49 for femoral hernia repair (n = 3); $120.90 ± $30.51 for umbilical hernia repair (n = 8); $36.59 ± $17.76 for minor procedures (n = 26); and $120.66 ± $14.61 for pediatric inguinal hernia repair (n = 7).
Conclusion: Supply acquisition at NPO costs leads to significant cost-savings compared with supply acquisition at US academic institution costs from the provider perspective for inguinal hernia repair, hydrocelectomy, umbilical hernia repair, minor procedures, and pediatric inguinal hernia repair during a surgical mission in the Dominican Republic. Item utilization analysis can generate minimum-necessary material lists for each procedure type to reproduce cost-savings for subsequent missions.
Figures
Similar articles
-
Variation in the use of laparoscopy with inguinal hernia repairs in a sample of pediatric patients at children's hospitals.J Pediatr Urol. 2018 Apr;14(2):158.e1-158.e7. doi: 10.1016/j.jpurol.2017.10.008. Epub 2017 Nov 29. J Pediatr Urol. 2018. PMID: 29195832
-
Cost-effectiveness of inguinal hernia surgery in northwestern Ecuador.World J Surg. 2013 Jan;37(1):32-41. doi: 10.1007/s00268-012-1808-5. World J Surg. 2013. PMID: 23073503
-
Emergency repair of inguinal hernia in the premature infant is associated with high direct medical costs.Hernia. 2016 Aug;20(4):571-7. doi: 10.1007/s10029-015-1447-5. Epub 2015 Dec 14. Hernia. 2016. PMID: 26667260 Free PMC article.
-
Sustainability in humanitarian surgery during medical short-term trips (MSTs): feasibility of inguinal hernia repair in rural Nigeria over 6 years and 13 missions.Hernia. 2018 Jun;22(3):491-498. doi: 10.1007/s10029-018-1758-4. Epub 2018 Mar 31. Hernia. 2018. PMID: 29605842
-
Medical mission to dominican republic: one dermatology group?s experiences.J Spec Oper Med. 2013 Summer;13(2):69-74. doi: 10.55460/QDLB-CR5Y. J Spec Oper Med. 2013. PMID: 23817882 Review.
Cited by
-
International guidelines for groin hernia management.Hernia. 2018 Feb;22(1):1-165. doi: 10.1007/s10029-017-1668-x. Epub 2018 Jan 12. Hernia. 2018. PMID: 29330835 Free PMC article.
-
A Systematic Review of Economic Analysis of Surgical Mission Trips Using the World Health Organization Criteria.World J Surg. 2016 Aug;40(8):1874-84. doi: 10.1007/s00268-016-3542-x. World J Surg. 2016. PMID: 27160452
-
Surgical outreach for the Americas: a self-sustainable model for partnership and education.Surg Endosc. 2024 Aug;38(8):4657-4662. doi: 10.1007/s00464-024-11015-2. Epub 2024 Jul 8. Surg Endosc. 2024. PMID: 38977500
References
-
- Weiser TG, Regenbogen SE, Thompson KD, Haynes AB, Lipsitz SR, Berry WR, Gawande AA. An estimation of the global volume of surgery: a modeling strategy based on available data. Lancet. 2008;372(9633):139–144. - PubMed
-
- Ozgediz D, Hsia R, Weiser T, Gosselin R, Spiegel D, Bickler S, Dunbar P, McQueen K. Population health metrics for surgery: effecive coverage of surgical services in low-income and middle-income countries. World J Surg. 2009;33(1):1–5. - PubMed
-
- Taira BR, McQueen KA, Burkle FM., Jr Burden of surgical disease: does the literature reflect the scope of the international crisis? World J Surg. 2009;33(5):893–898. - PubMed
-
- Debas HT, Gosselin R, McCord C, Surgery Thind A. Disease Control Priorities in Developing Countries. In: Jamison DT, Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB, Jha P, Mills A, Musgrove P, editors. Disease Control Priorities Project. 2nd ed. Washington, DC: International Bank for Reconstruction and Development/World Bank; 2006. pp. 1245–1260. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
