

Review
doi: 10.3978/j.issn.2072-1439.2013.07.27.
Modern diagnostic and therapeutic interventional radiology in lung cancer
Affiliations
- PMID: 24163744
- PMCID: PMC3804882
- DOI: 10.3978/j.issn.2072-1439.2013.07.27
Item in Clipboard
Review
Modern diagnostic and therapeutic interventional radiology in lung cancer
J Thorac Dis.
2013 Oct.
Abstract
Imaging has an important role in the multidisciplinary management of primary lung cancer. This article reviews the current state-of-the-art imaging modalities used for the evaluation, staging and post-treatment follow-up and surveillance of lung cancers, and image-guided percutaneous techniques for biopsy to confirm the diagnosis and for local therapy in non-surgical candidates.
Keywords: Lung neoplasms; ablation; biopsy; computed tomography (CT); magnetic resonance (MR); positron emission tomography (PET)/CT.
Figures
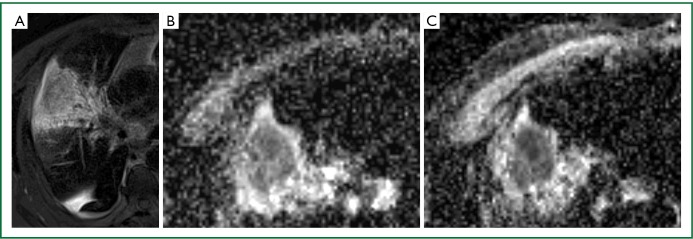
A 71-year-old man with Stage III NSCLC in the right upper lobe. A. Axial T2-weighted MR image shows a heterogeneous T2 hyperintense mass with surrounding atelectasis; B, C. Axial ADC diffusion images before (B) and 24 hours after (C) starting chemotherapy show reduced ADC signal intensity in tumour following treatment.
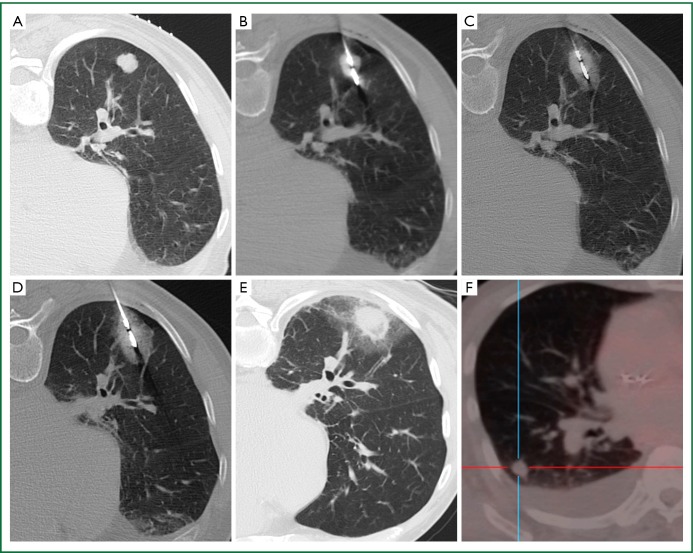
A 70-year-old man with cardiomyopathy and new solitary melanoma metastasis to the right lower lobe. A. Prone axial CT image shows a lobulated 1.6 cm tumour; B. The feed point of the microwave antenna is positioned within the centre of the tumour; C, D. At 5 minutes following the start of ablation (C), there is ground glass opacity forming mainly on the far edge of the tumour, and at 10 minutes (D), a 3-10 mm circumferential rim of ground glass opacity has formed around the tumour; E. At 3 hours following ablation, there is marked (>1 cm) circumferential ground glass opacity around the tumour; F. Axial FDG-PET/CT image 6 months following MWA shows complete lack of FDG uptake at the site of tumour, indicating eradication of tumour. New cardiac-related pleural effusion is present.
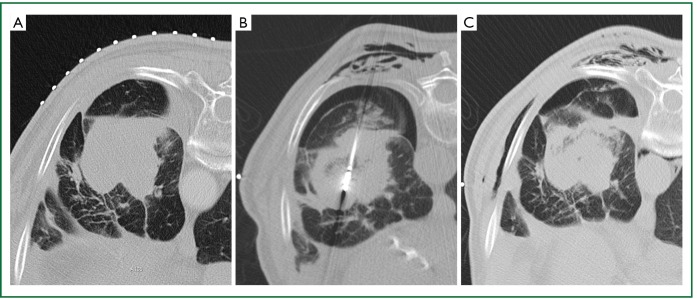
A 72-year-old man with incomplete response to external beam radiation to left lower lobe NSCLC, who presented for salvage MWA. He had an intractable cough throughout the procedure. A. Prone axial CT image shows a 5.5 cm mass before MWA; B. Prone axial CT during the procedure shows a small pneumothorax and surgical emphysema developing around the antenna entry site; C. Prone axial CT at the end of the procedure shows the pneumothorax has remained similar in size, but there is increased surgical emphysema.

A 75-year-old ex-smoker with prior RFA of biopsy-proven left upper lobe NSCLC. FDG-PET 3 months following RFA was equivocal for residual tumour and repeat treatment with CT-guided MWA was performed. A. Axial CT image shows a 3 cm left upper lobe mass; B. Axial CT shows microwave antenna is positioned within the centre of the mass; C. Axial CT 24 hours following MWA shows ablation site encompasses target lesion. There is a focal pleural effusion with small cavity, and surrounding atelectasis and ground glass opacity changes; D, E. Axial CT (D) and axial fused FDG-PET/CT (E) 6 months following ablation show resolution of the ground glass opacity and shrinking of the ablation volume, but a residual broad-based pleural contact remain. FDG-PET/CT shows lack of FDG-avidity of the ablated lesion but mild sub-pleural FDG uptake, likely inflammatory; F, G. Axial CT 12 months (F) and 24 months (G) following ablation show further gradual shrinking of the ablation volume and narrowing of the pleural contact.
References
-
- Ravenel JG, Mohammed TL, Movsas B, et al. ACR Appropriateness Criteria® noninvasive clinical staging of bronchogenic carcinoma. J Thorac Imaging 2010;25:W107-11. - PubMed
-
- Willemink MJ, Leiner T, de Jong PA, et al. Iterative reconstruction techniques for computed tomography part 2: initial results in dose reduction and image quality. Eur Radiol 2013;23:1632-42 - PubMed
-
- Vardhanabhuti V, Loader RJ, Mitchell GR, et al. Image quality assessment of standard- and low-dose chest CT using filtered back projection, adaptive statistical iterative reconstruction, and novel model-based iterative reconstruction algorithms. AJR Am J Roentgenol 2013;200:545-52 - PubMed
-
- Walsh SL, Nair A, Hansell DM. Post-processing applications in thoracic computed tomography. Clin Radiol 2013;68:433-48 - PubMed
-
- Stoelben E, Ludwig C.Chest wall resection for lung cancer: indications and techniques. Eur J Cardiothorac Surg 2009;35:450-6 - PubMed
Publication types
LinkOut - more resources
Full Text Sources