

Surgery in 2013 and beyond
- PMID: 24163751
- PMCID: PMC3804869
- DOI: 10.3978/j.issn.2072-1439.2013.07.39
Surgery in 2013 and beyond
Abstract
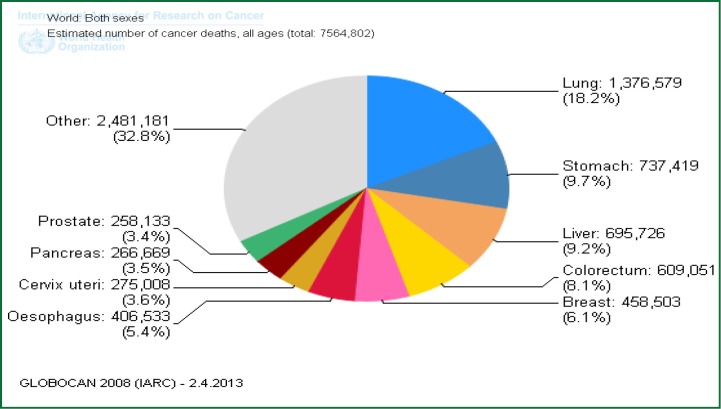
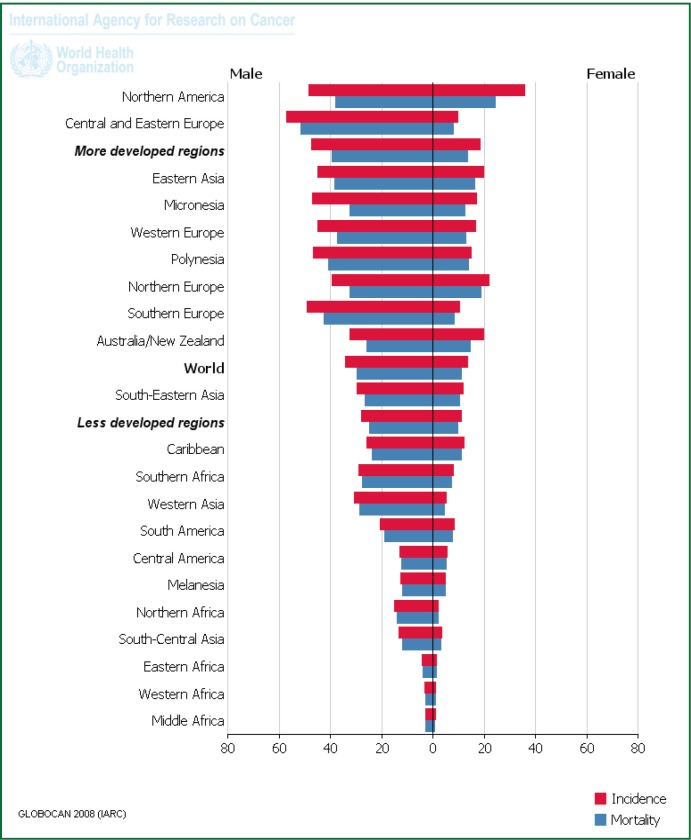
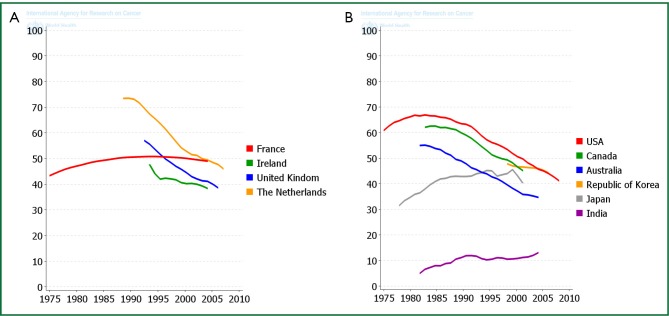
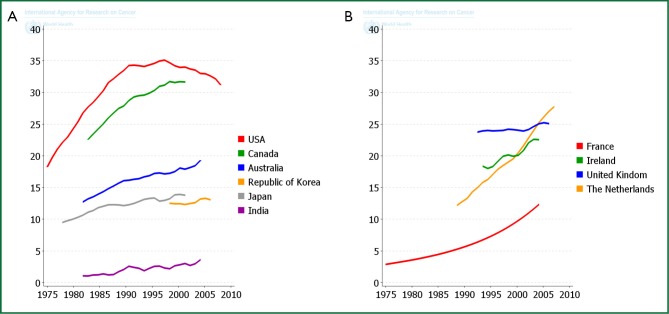
Lung cancer is a leading cause of cancer related mortality. The role of surgery continues to evolve and in the last ten years there have been a number of significant changes in the surgical management of lung cancer. These changes extend across the entire surgical spectrum of lung cancer management including diagnosis, staging, treatment and pathology. Positron Emission Tomography (PET) scanning and ultrasound (EBUS) have redefined traditional staging paradigms, and surgical techniques, including video-assisted thoracoscopy (VATS), robotic surgery and uniportal surgery, are now accepted as standard of care in many centers. The changing pathology of lung cancer, with more peripheral tumours and an increase in adenocarcinomas has important implications for the Thoracic surgeon. Screening, using Low-Dose CT scanning, is having an impact, with not only a higher percentage of lower stage cancers detected, but also redefining the role of sublobar resection. The incidence of pneumonectomy has reduced as have the rates of "exploratory thoracotomy". In general, lung resection is considered for stage I and II patients with a selected role in more advanced stage disease as part of a multimodality approach. This paper will look at these issues and how they impact on Thoracic Surgical practice in 2013 and beyond.
Keywords: Lung cancer; surgery.
Figures
References
-
- Ferlay J, Shin HR, Bray F, et al. GLOBOCAN 2008 v2.0, Cancer incidence and mortality worldwide: IARC CancerBase No. 10 (Internet). Lyon, France: International Agency for Research on Cancer; 2010. Available online: http://globocan.iarc.fr, accessed on 7/04/2013.
-
- Australian Institute of Health and Welfare & Australasian Association of Cancer Registries 2012. Cancer in Australia: an overview, 2012. Cancer series no. 74. Cat. no. CAN 70. Canberra: AIHW.
-
- Australian Institute of Health and Welfare 2012. Cancer survival and prevalence in Australia: period estimates from 1982 to 2010. Cancer series no. 69. Cat. No. CAN 65. Canberra: AIHW. - PubMed
-
- Drilon A, Rekhtman N, Ladanyi M, et al. Squamous-cell carcinomas of the lung: emerging biology, controversies, and the promise of targeted therapy. Lancet Oncol 2012;13:e418-26 - PubMed
-
- Rekhtman N, Brandt SM, Sigel CS, et al. Suitability of thoracic cytology for new therapeutic paradigms in non-small cell lung carcinoma: high accuracy of tumor subtyping and feasibility of EGFR and KRAS molecular testing. J Thorac Oncol 2011;6:451-8 - PubMed
Publication types
LinkOut - more resources
Full Text Sources