

Serum biomarkers of brain injury to classify outcome after pediatric cardiac arrest*
- PMID: 24164954
- PMCID: PMC4478619
- DOI: 10.1097/01.ccm.0000435668.53188.80
Serum biomarkers of brain injury to classify outcome after pediatric cardiac arrest*
Abstract
Objectives: Morbidity and mortality in children with cardiac arrest largely result from neurologic injury. Serum biomarkers of brain injury can potentially measure injury to neurons (neuron-specific enolase), astrocytes (S100b), and axons (myelin basic protein). We hypothesized that serum biomarkers can be used to classify outcome from pediatric cardiac arrest.
Design: Prospective observational study.
Setting: Single tertiary pediatric hospital.
Patients: Forty-three children with cardiac arrest.
Interventions: None.
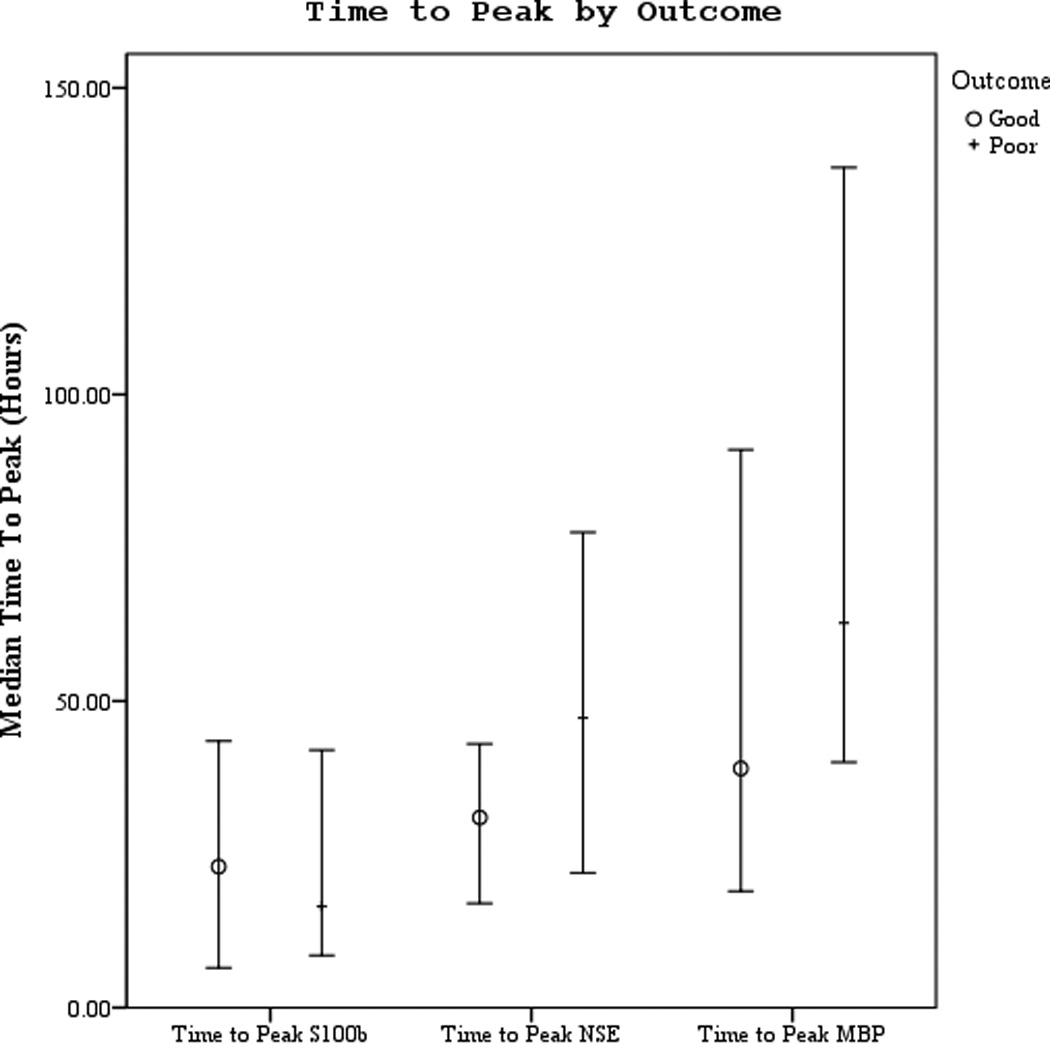
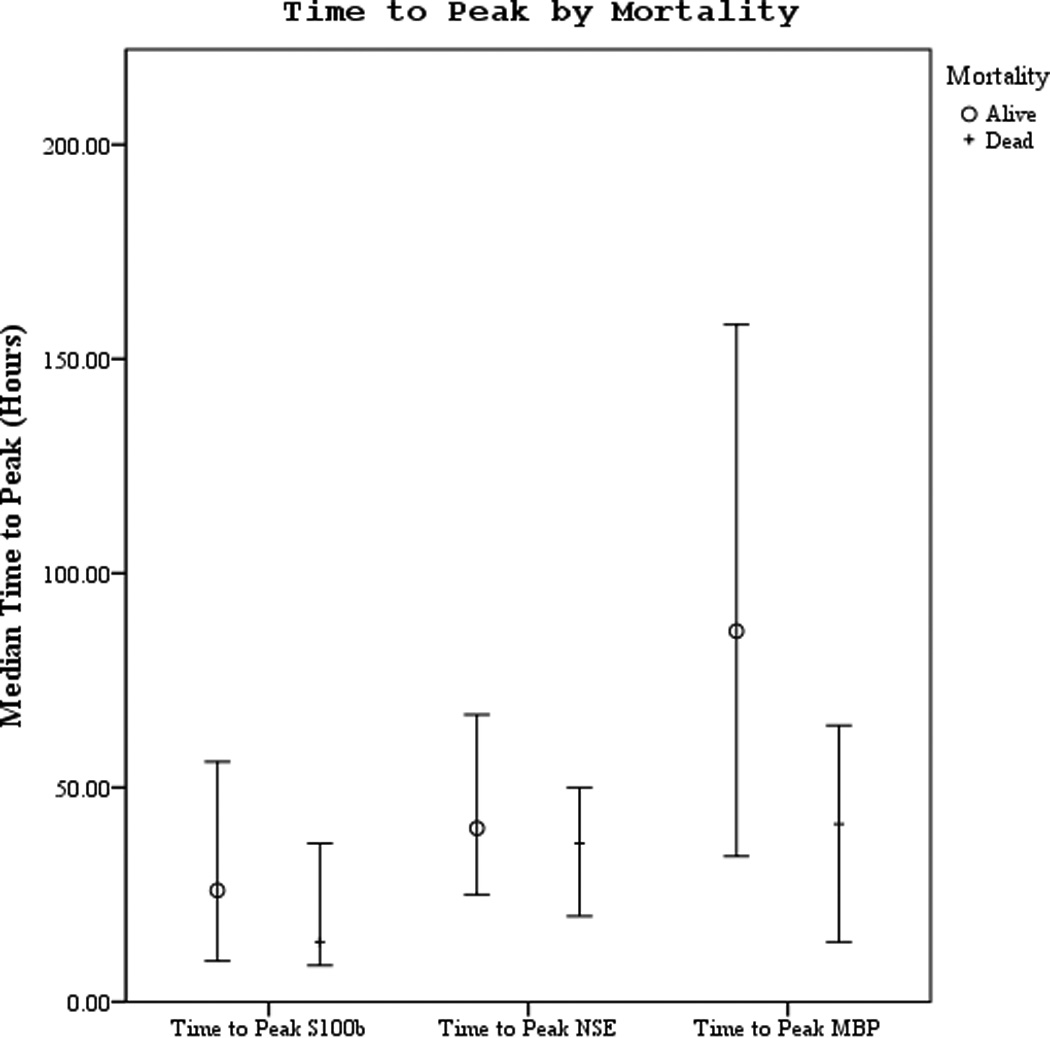
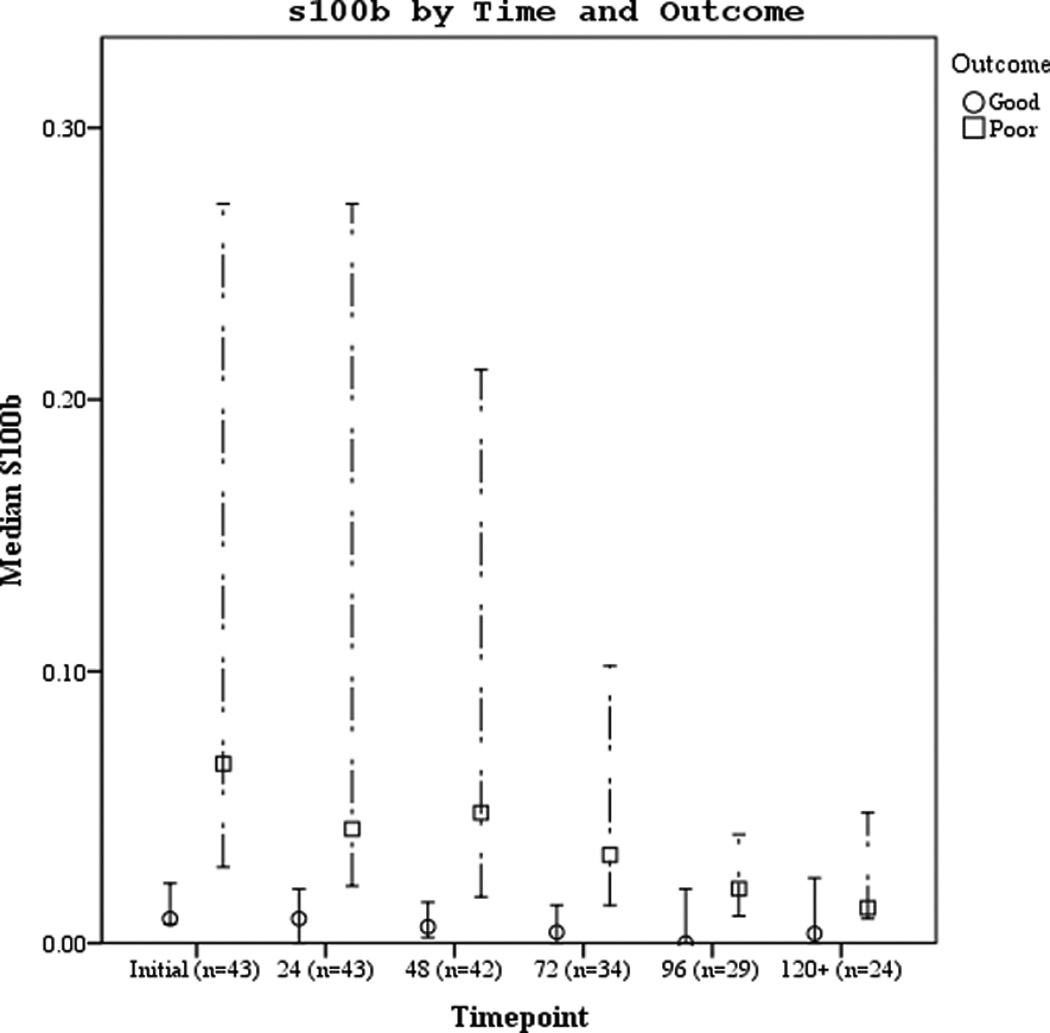
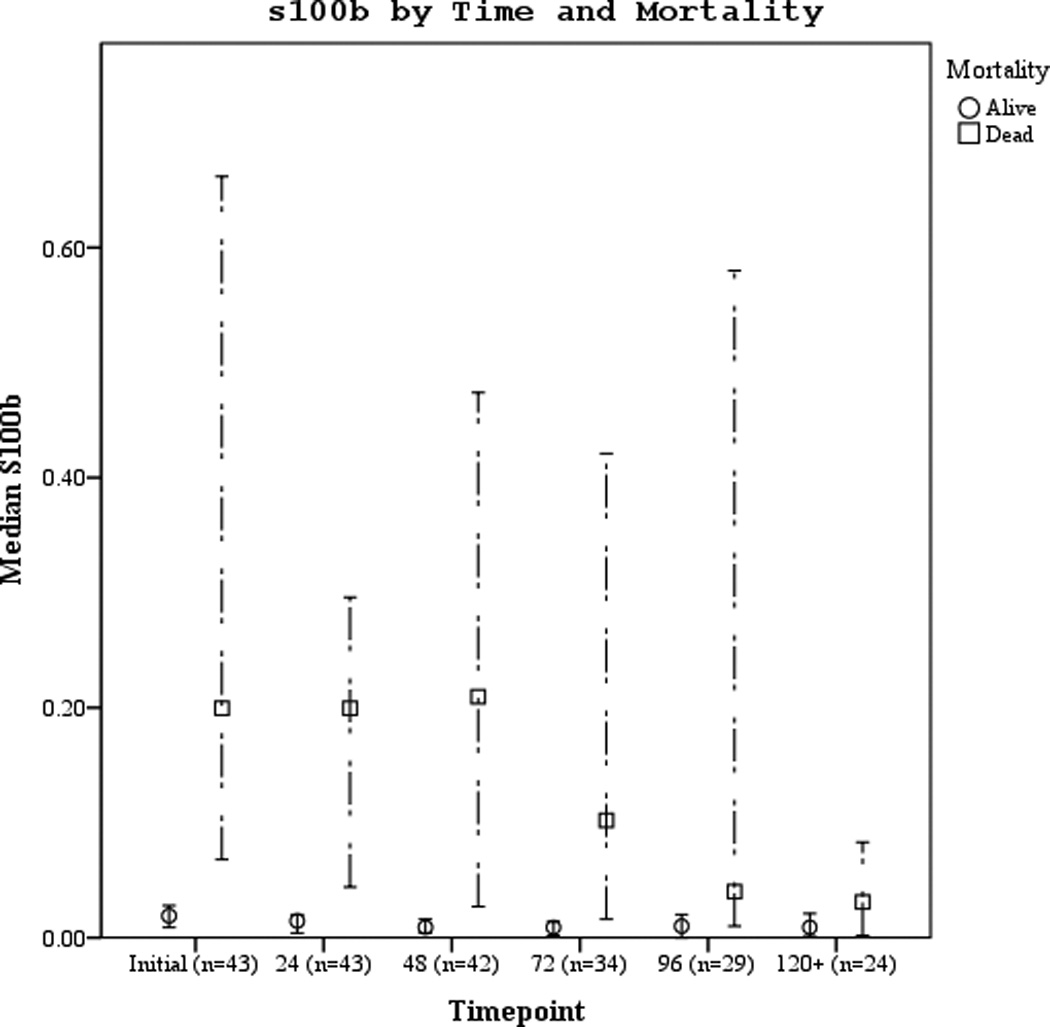
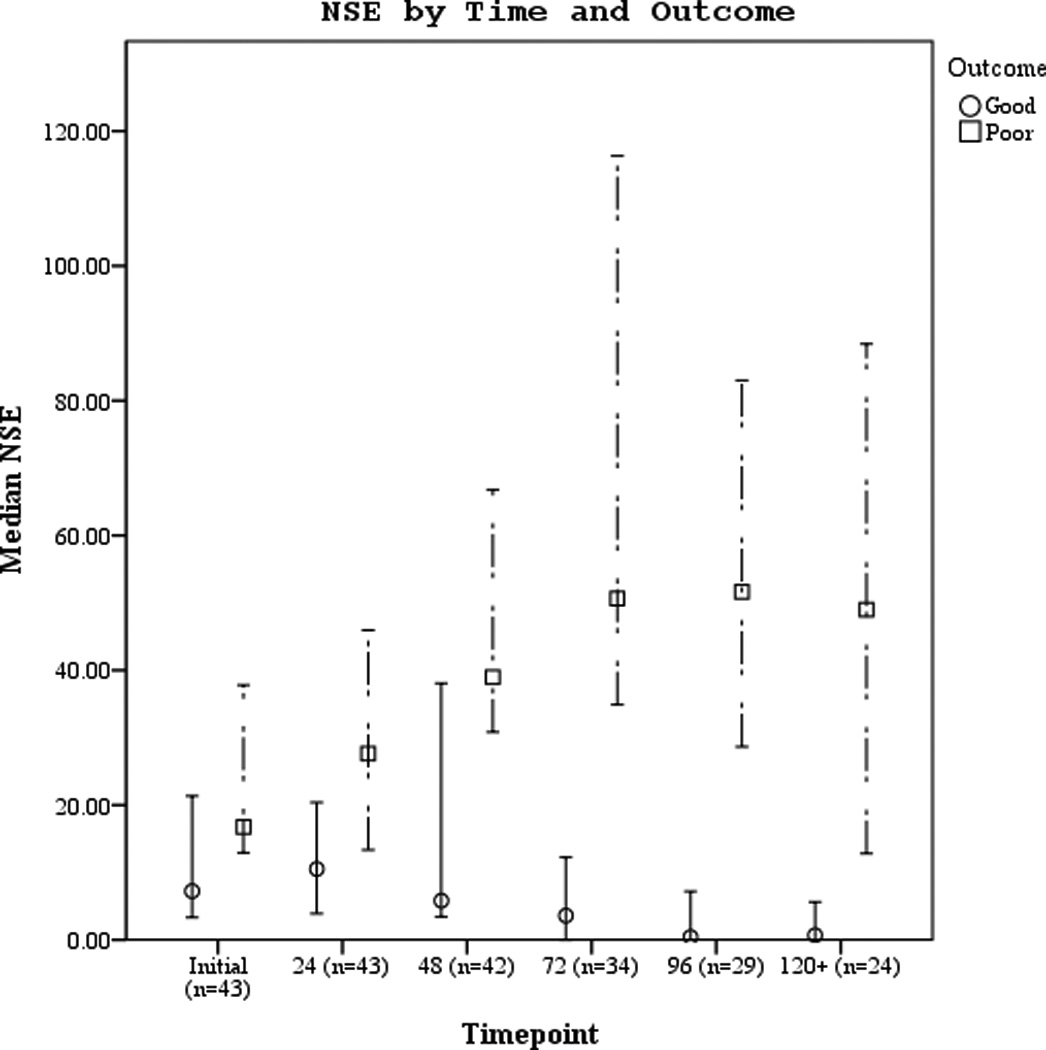
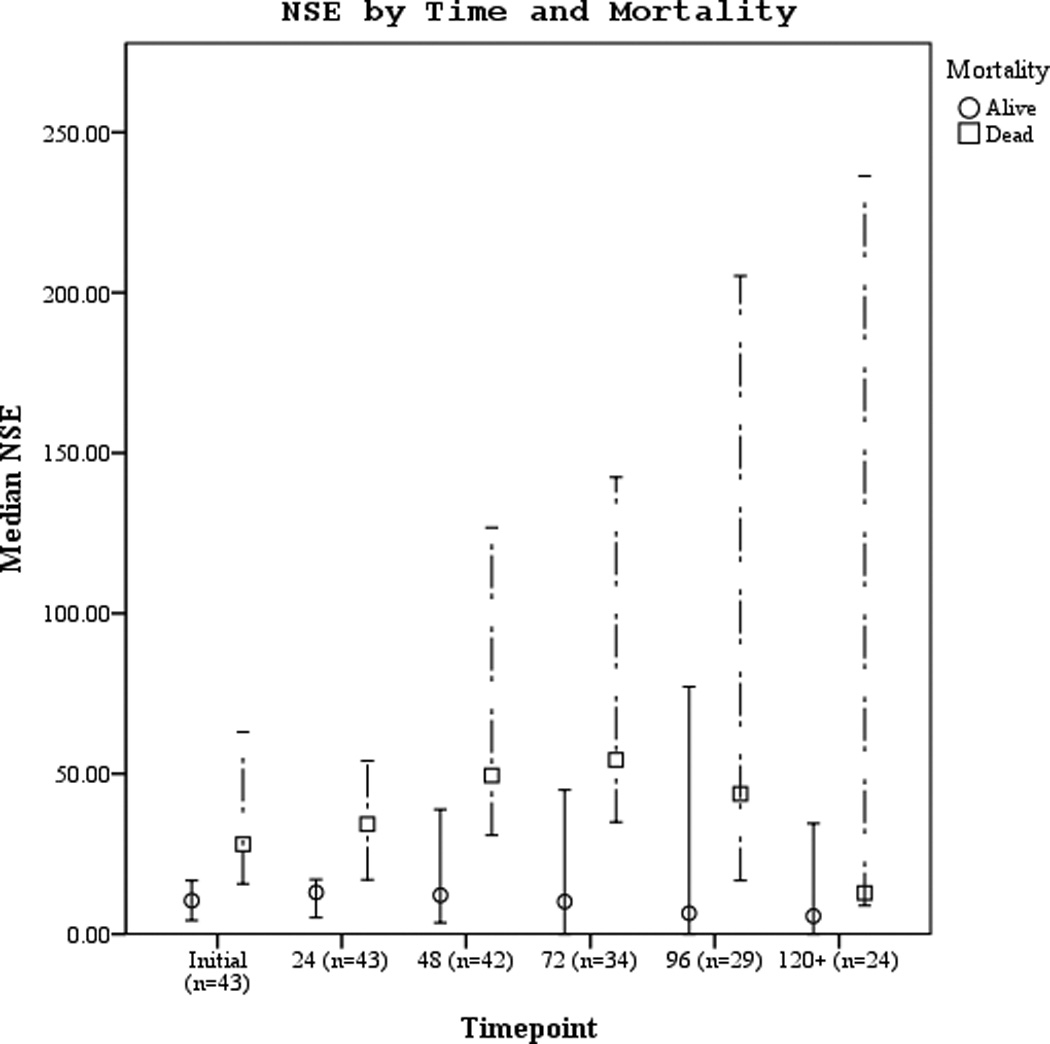
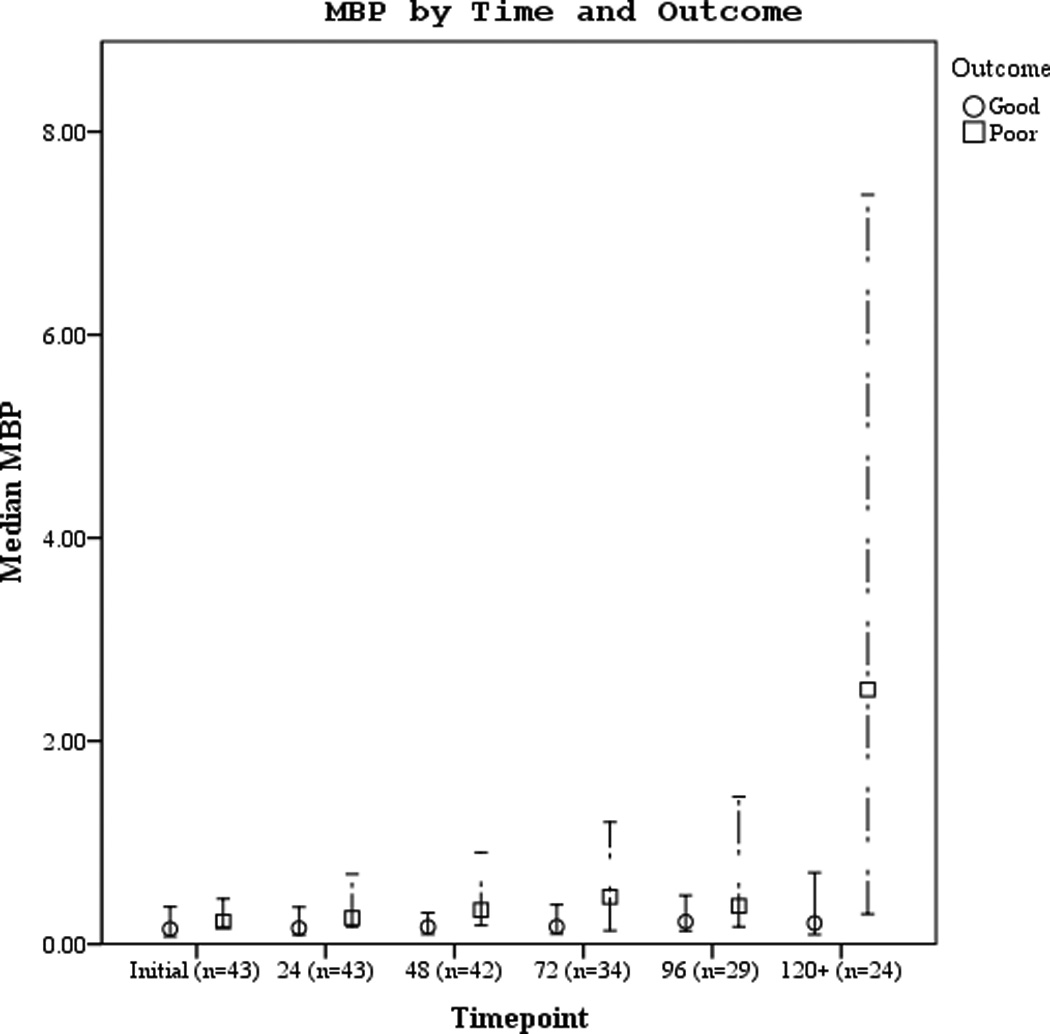
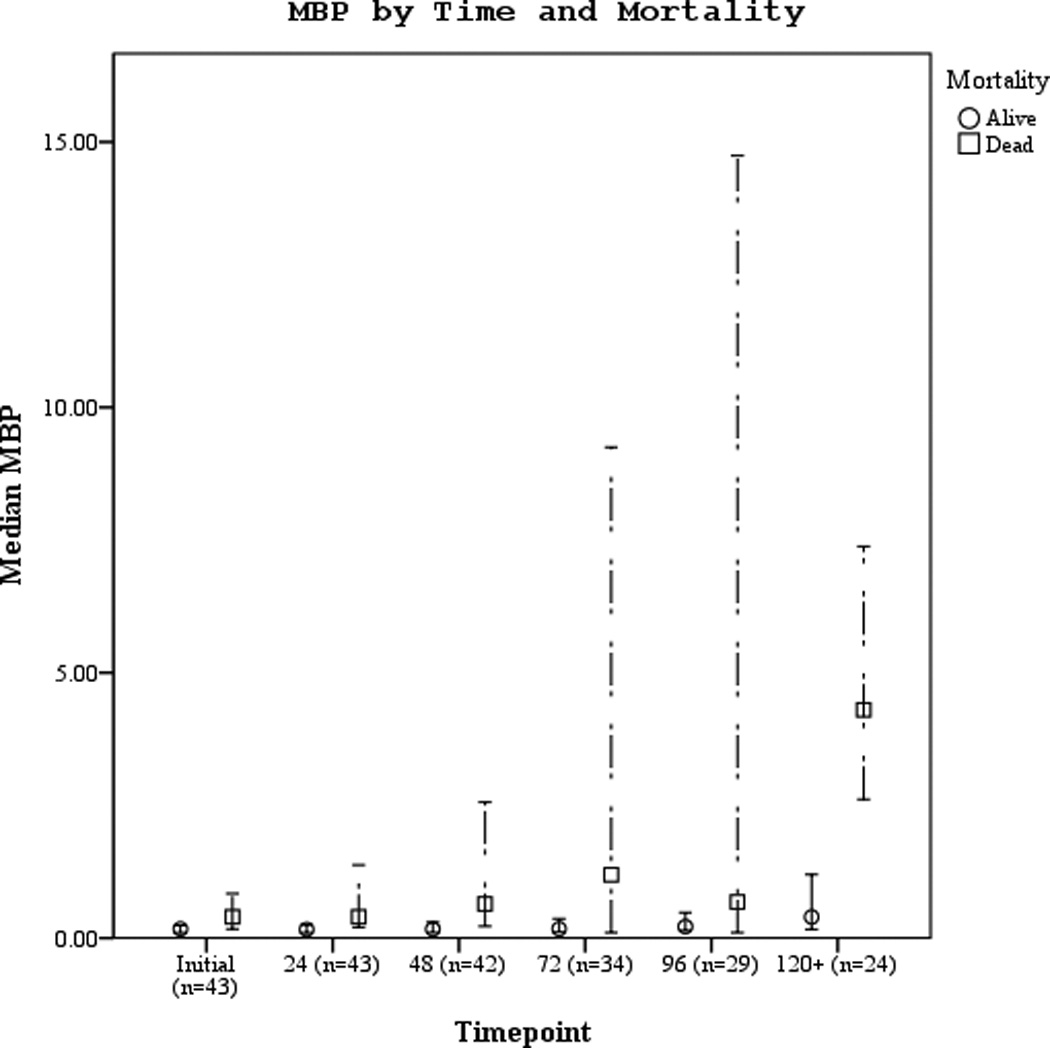
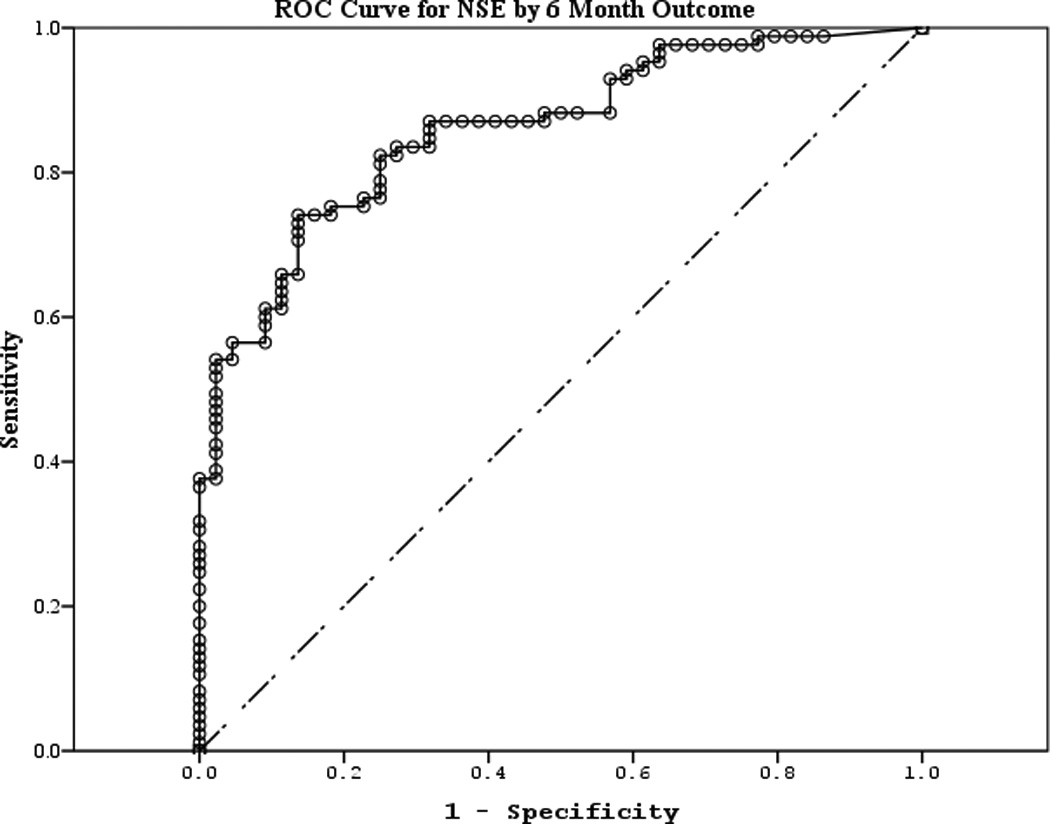
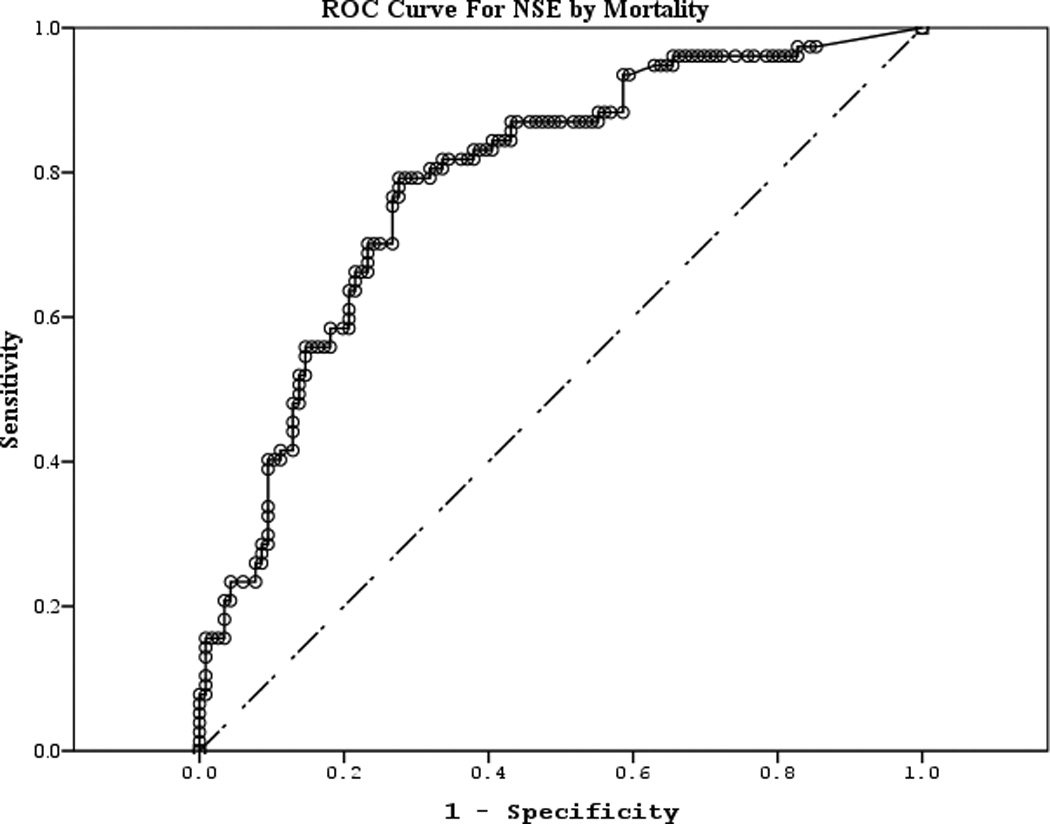
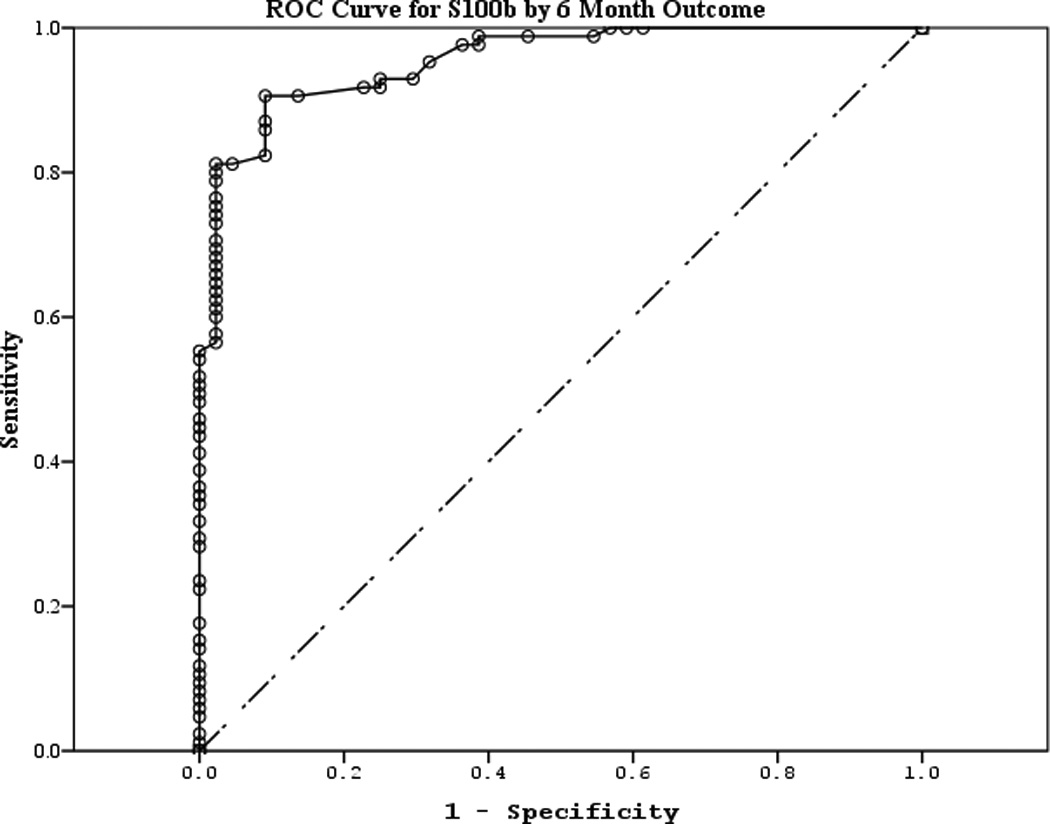
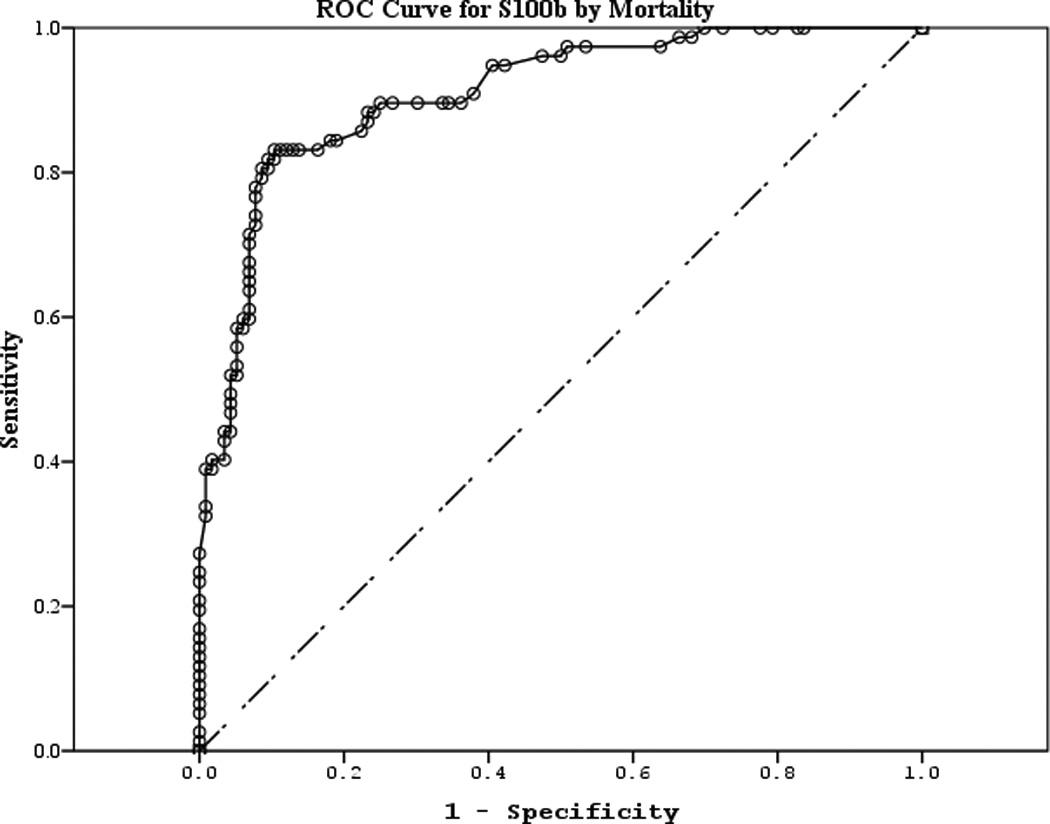
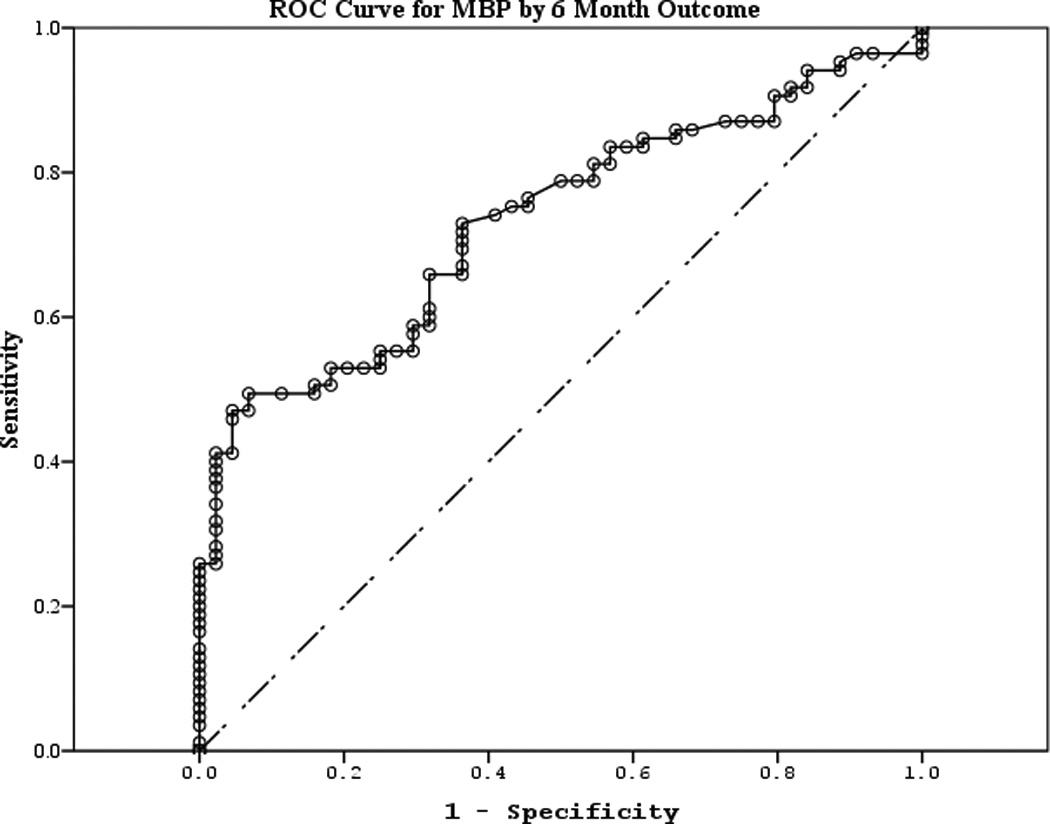
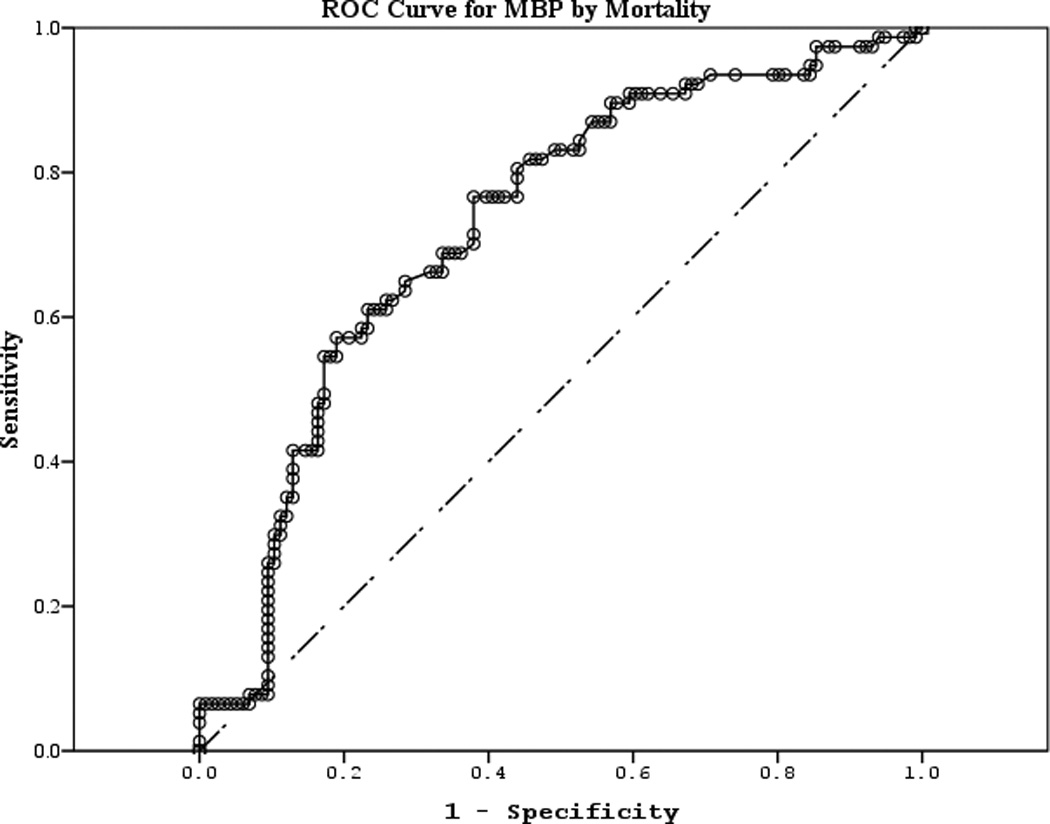
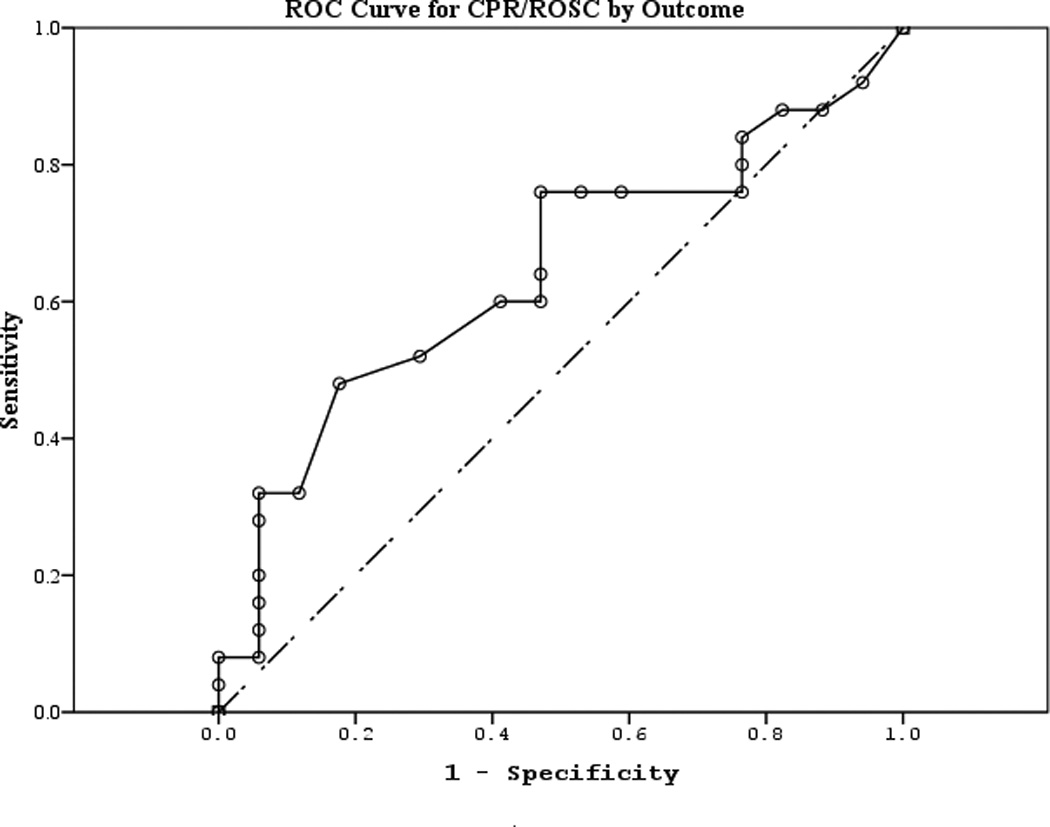
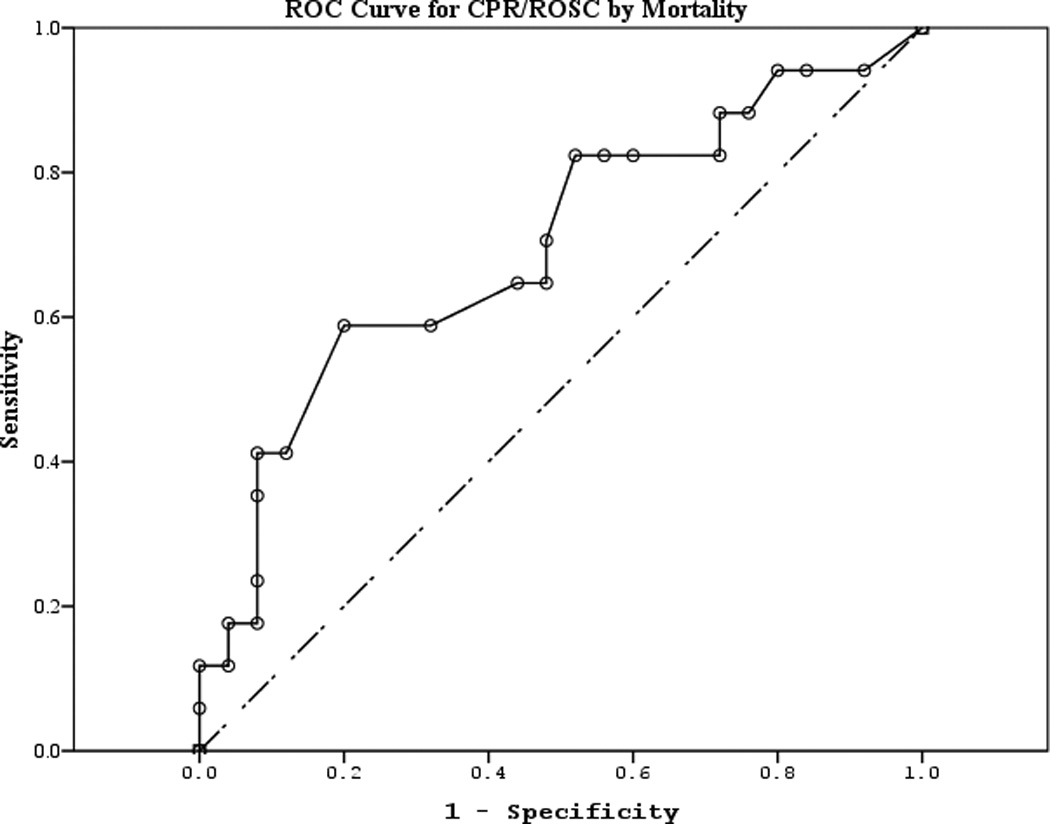
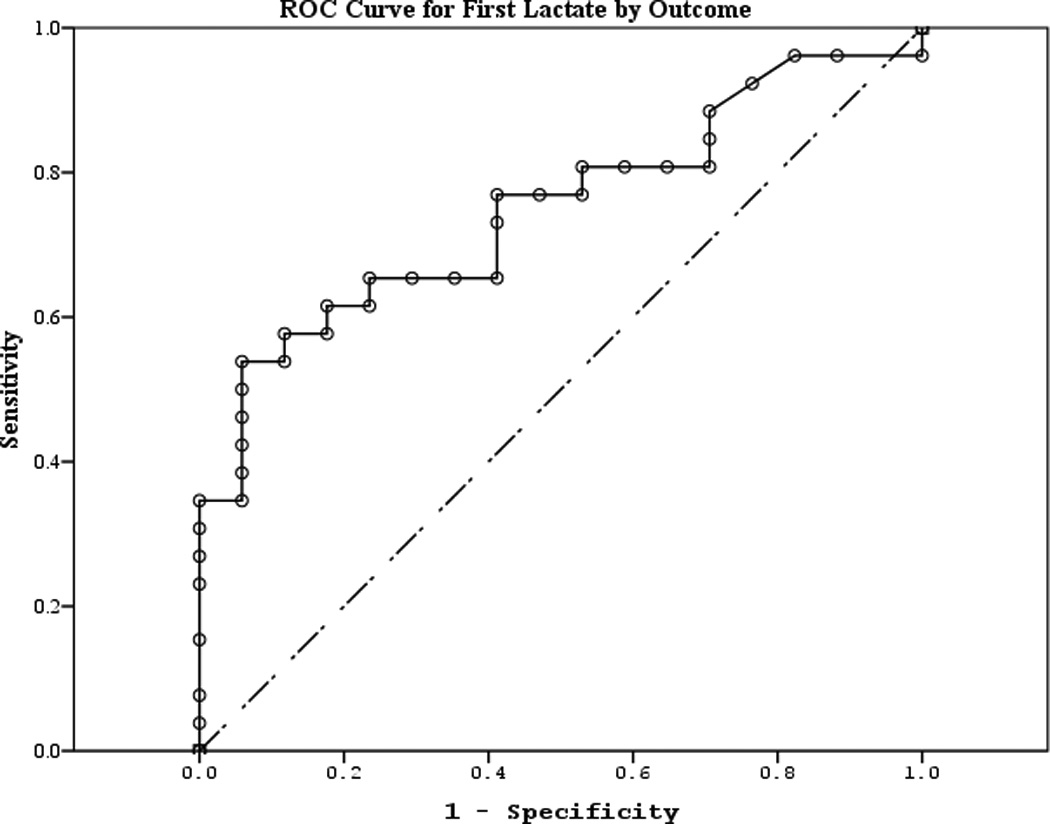
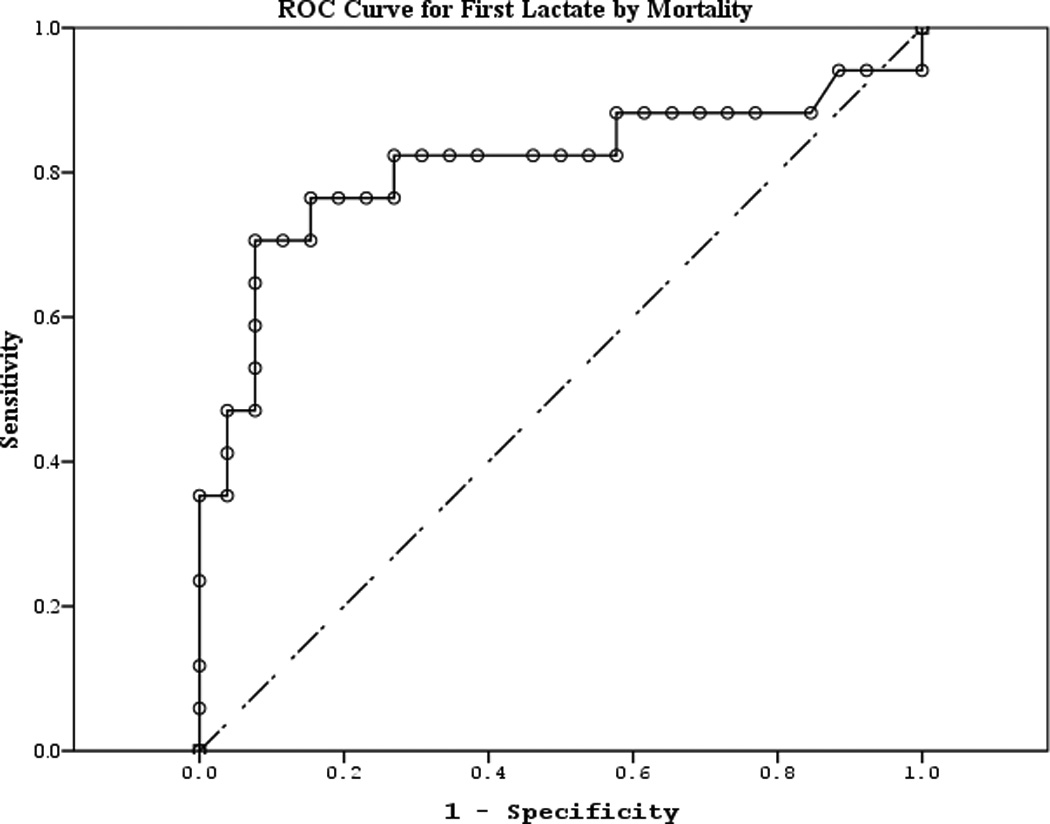
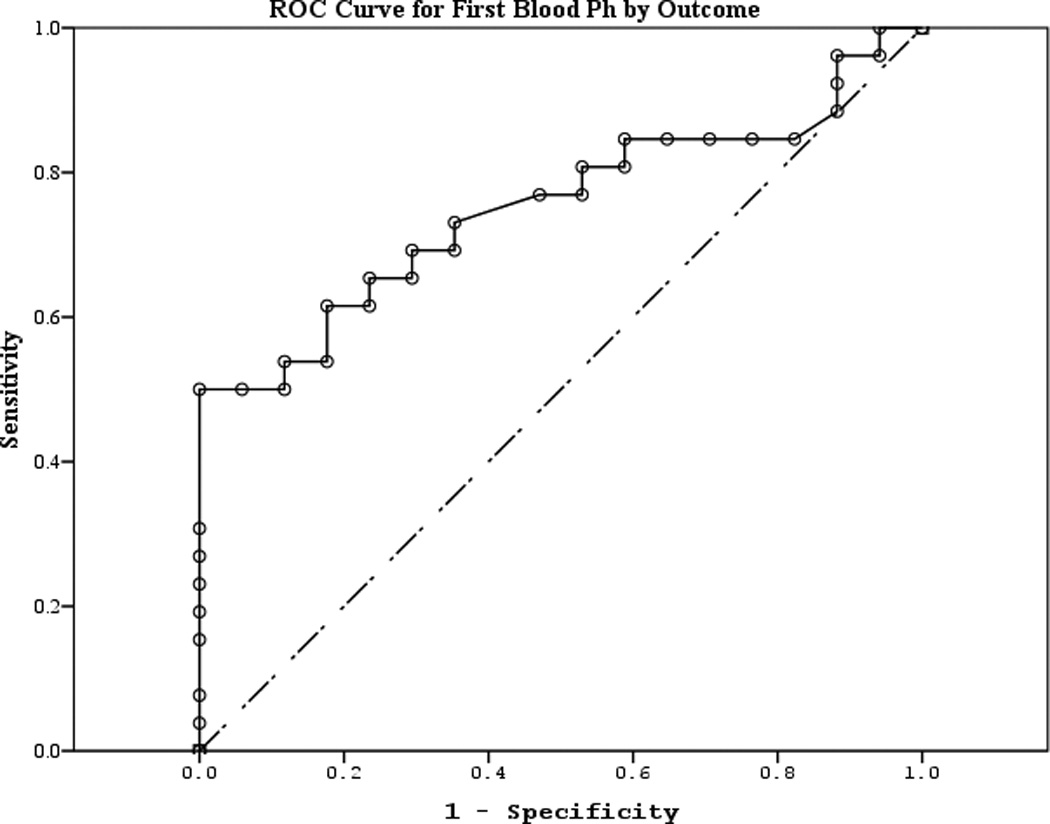
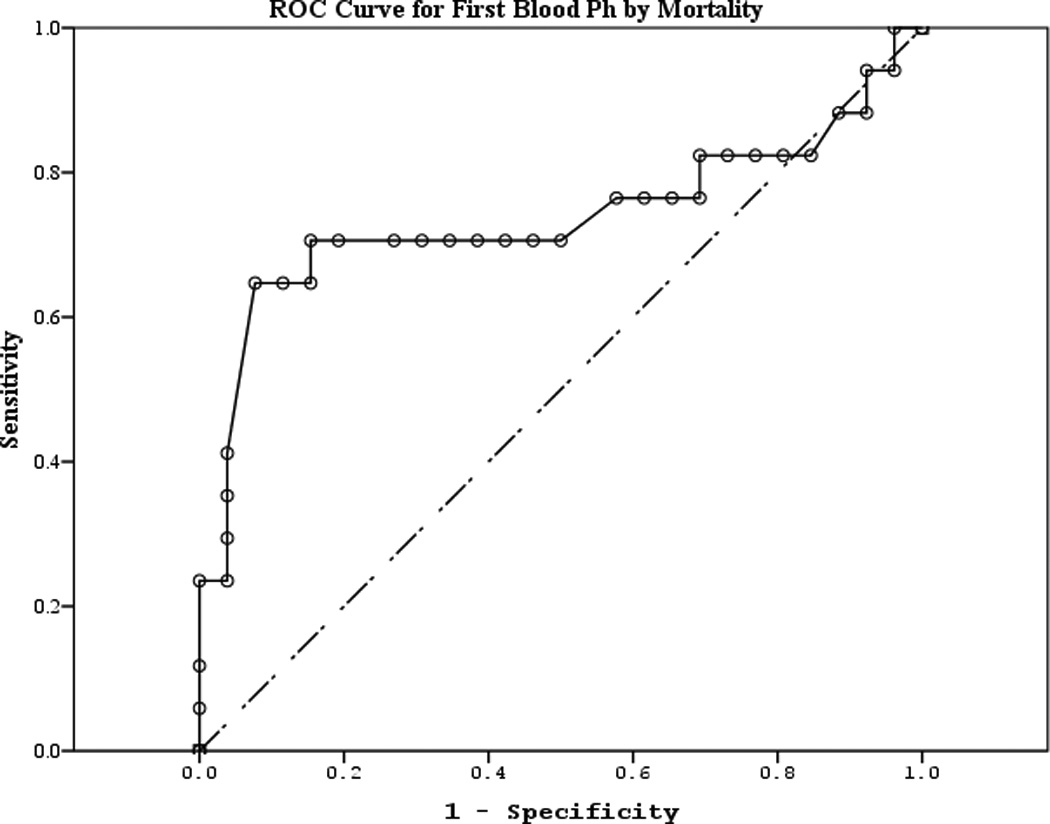
Measurements and main results: We measured serum neuron-specific enolase, S100b, and myelin basic protein on days 1-4 and 7 after cardiac arrest. We recorded demographics, details of the cardiac arrest and resuscitation, and Pediatric Cerebral Performance Category at hospital discharge and 6 months. We analyzed the association of biomarker levels at 24, 48, and 72 hours with favorable (Pediatric Cerebral Performance Category 1-3) or unfavorable (Pediatric Cerebral Performance Category 4-6) outcome and mortality. Forty-three children (49% female; mean age of 5.9 ± 6.3) were enrolled and 17 (40%) died. Serum S100b concentrations peaked earliest, followed by neuron-specific enolase and finally myelin basic protein. Serum neuron-specific enolase and S100b concentrations were increased in the unfavorable versus favorable outcome group and in subjects who died at all time points (all p < 0.05). Serum myelin basic protein at 24 and 72 hours correctly classified survival but not good versus poor outcome. Using best specificity, serum S100b and neuron-specific enolase had optimal positive and negative predictive values at 24 hours to classify both favorable versus unfavorable outcome and survival, whereas serum myelin basic protein's best accuracy occurred at 48 hours. Receiver operator curves for serum S100b and neuron-specific enolase to classify favorable versus unfavorable outcome at 6 months were superior to clinical variables.
Conclusions: Preliminary data show that serum S100b, neuron-specific enolase, and myelin basic protein may aid in outcome classification of children surviving cardiac arrest.
Figures
Comment in
-
Are we any closer to predicting outcomes of pediatric cardiac arrest?*.Crit Care Med. 2014 Mar;42(3):753-4. doi: 10.1097/CCM.0000000000000066. Crit Care Med. 2014. PMID: 24534973 No abstract available.
References
-
- Kuisma M, Suominen P, Korpela R. Paediatric out-of-hospital cardiac arrests--epidemiology and outcome. Resuscitation. 1995 Oct;30(2):141–150. - PubMed
-
- Reis AG, Nadkarni V, Perondi MB, Grisi S, Berg RA. A prospective investigation into the epidemiology of in-hospital pediatric cardiopulmonary resuscitation using the international Utstein reporting style. Pediatrics. 2002;109(2):200–209. - PubMed
-
- Young KD, Gausche-Hill M, McClung CD, Lewis RJ. A prospective, population-based study of the epidemiology and outcome of out-of-hospital pediatric cardiopulmonary arrest. Pediatrics. 2004 Jul;114(1):157–164. - PubMed
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA. 2006 Jan 4;295(1):50–57. - PubMed
-
- de Mos N, van Litsenburg RR, McCrindle B, Bohn DJ, Parshuram CS. Pediatric in-intensive-care-unit cardiac arrest: incidence, survival, and predictive factors. Crit Care Med. 2006 Apr;34(4):1209–1215. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
