

Ultrasound mapping of pelvic endometriosis: does the location and number of lesions affect the diagnostic accuracy? A multicentre diagnostic accuracy study
- PMID: 24165087
- PMCID: PMC3815071
- DOI: 10.1186/1472-6874-13-43
Ultrasound mapping of pelvic endometriosis: does the location and number of lesions affect the diagnostic accuracy? A multicentre diagnostic accuracy study
Abstract
Background: Endometriosis is a common condition which causes pain and reduced fertility. Treatment can be difficult, especially for severe disease, and an accurate preoperative assessment would greatly help in the managment of these patients. The objective of this study is to assess the accuracy of pre-operative transvaginal ultrasound scanning (TVS) in identifying the specific features of pelvic endometriosis and pelvic adhesions in comparison with laparoscopy.
Methods: Consecutive women with clinically suspected or proven pelvic endometriosis, who were booked for laparoscopy, were invited to join the study. They all underwent a systematic transvaginal ultrasound examination in order to identify discrete endometriotic lesions and pelvic adhesions. The accuracy of ultrasound diagnosis was determined by comparing pre-operative ultrasound to laparoscopy findings.
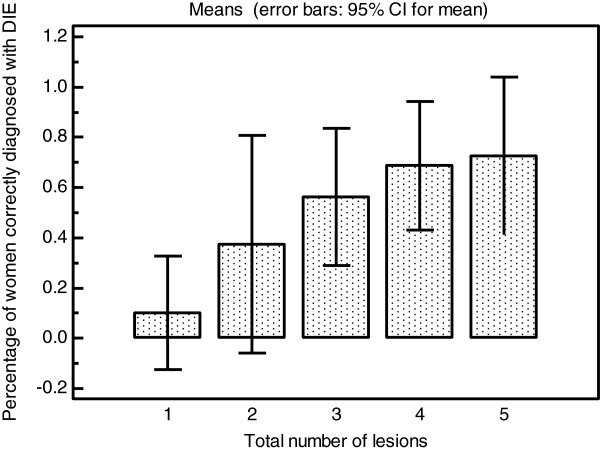
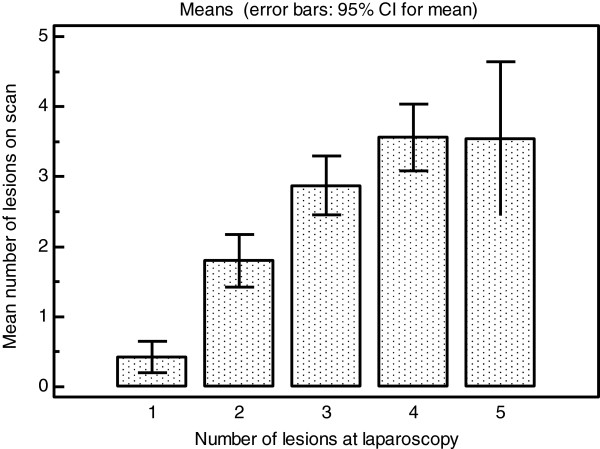
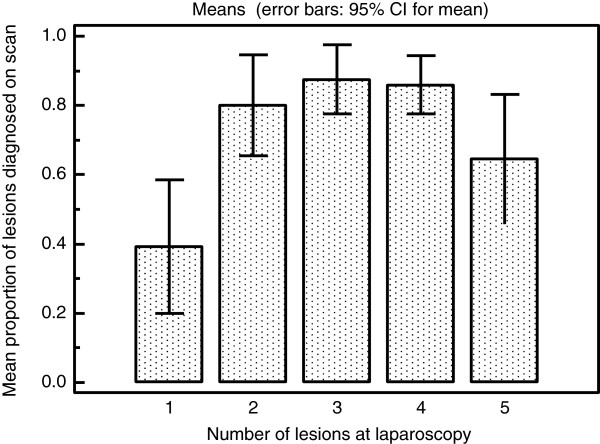
Results: 198 women who underwent preoperative TVS and laparoscopy were included in the final analysis. At laparoscopy 126/198 (63.6%) women had evidence of pelvic endometriosis. 28/126 (22.8%) of them had endometriosis in a single location whilst the remaining 98/126 (77.2%) had endometriosis in two or more locations. Positive likelihood ratios (LR+) for the ultrasound diagnosis of ovarian endometriomas, moderate or severe ovarian adhesions, pouch of Douglas adhesions, and bladder deeply infiltrating endometriosis (DIE), recto-sigmoid colon DIE, rectovaginal DIE, uterovesical fold DIE and uterosacral ligament DIE were >10, whilst for pelvic side wall DIE and any ovarian adhesions the + LH was 8.421 and 9.81 respectively.The negative likelihood ratio (LR-) was: <0.1 for bladder DIE; 0.1-0.2 for ovarian endometriomas, moderate or severe ovarian adhesions, and pouch of Douglas adhesions; 0.5-1 for rectovaginal, uterovesical fold, pelvic side wall and uterosacral ligament DIE. The accuracy of TVS for the diagnosis of both total number of endometriotic lesions and DIE lesions significantly improved with increasing total number of lesions.
Conclusions: Our study has shown that the TVS diagnosis of endometriotic lesion is very specific and false positive results are rare. Negative findings are less reliable and women with significant symptoms may still benefit from further investigation even if TVS findings are normal. The accuracy of ultrasound diagnosis is significantly affected by the location and number of endometriotic lesions.
Figures
References
-
- Okaro E, Condous G, Khalid A, Timmerman D, Ameye L, Huffel SV, Bourne T. The use of ultrasound-based 'soft markers’ for the prediction of pelvic pathology in women with chronic pelvic pain–can we reduce the need for laparoscopy? BJOG. 2006;113:251–256. doi: 10.1111/j.1471-0528.2006.00849.x. - DOI - PubMed
-
- RCOG guideline. The investigation and management of endometriosis. Green top Guidel. 2006;24 [ http://www.rcog.org.uk/files/rcog-corp/GTG2410022011.pdf]
-
- Van Holsbeke C, Van Calster B, Guerriero S, Savelli L, Paladini D, Lissoni AA, Czekierdowski A, Fischerova D, Zhang J, Mestdagh G, Testa AC, Bourne T, Valentin L, Timmerman D. Endometriomas: their ultrasound characteristics. Ultrasound Obstet Gynecol. 2010;35:730–740. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
