

Improved acylated ghrelin suppression at 2 years in obese patients with type 2 diabetes: effects of bariatric surgery vs standard medical therapy
- PMID: 24166065
- PMCID: PMC4461212
- DOI: 10.1038/ijo.2013.196
Improved acylated ghrelin suppression at 2 years in obese patients with type 2 diabetes: effects of bariatric surgery vs standard medical therapy
Abstract
Objective: Roux-en-Y gastric bypass (RYGB) produces more durable glycemic control than sleeve gastrectomy (SG) or intensive medical therapy (IMT). However, the contribution of acylated ghrelin (AG), a gluco-regulatory/appetite hormone, to improve glucose metabolism and body composition in patients with type 2 diabetes (T2D) following RYGB is unknown.
Design: STAMPEDE (Surgical Treatment and Medication Potentially Eradicate Diabetes Efficiently) was a prospective, randomized controlled trial.
Subjects: Fifty-three (body mass index: 36±3 kg m(-2), age: 49±9 years) poorly controlled patients with T2D (HbA1c (glycated hemoglobin): 9.7±2%) were randomized to IMT, IMT+RYGB or IMT+SG and underwent a mixed-meal tolerance test at baseline, 12, and 24 months for evaluation of AG suppression (postprandial minus fasting) and beta-cell function (oral disposition index; glucose-stimulated insulin secretion × Matsuda index). Total/android body fat (dual-energy X-ray absorptiometry) was also assessed.
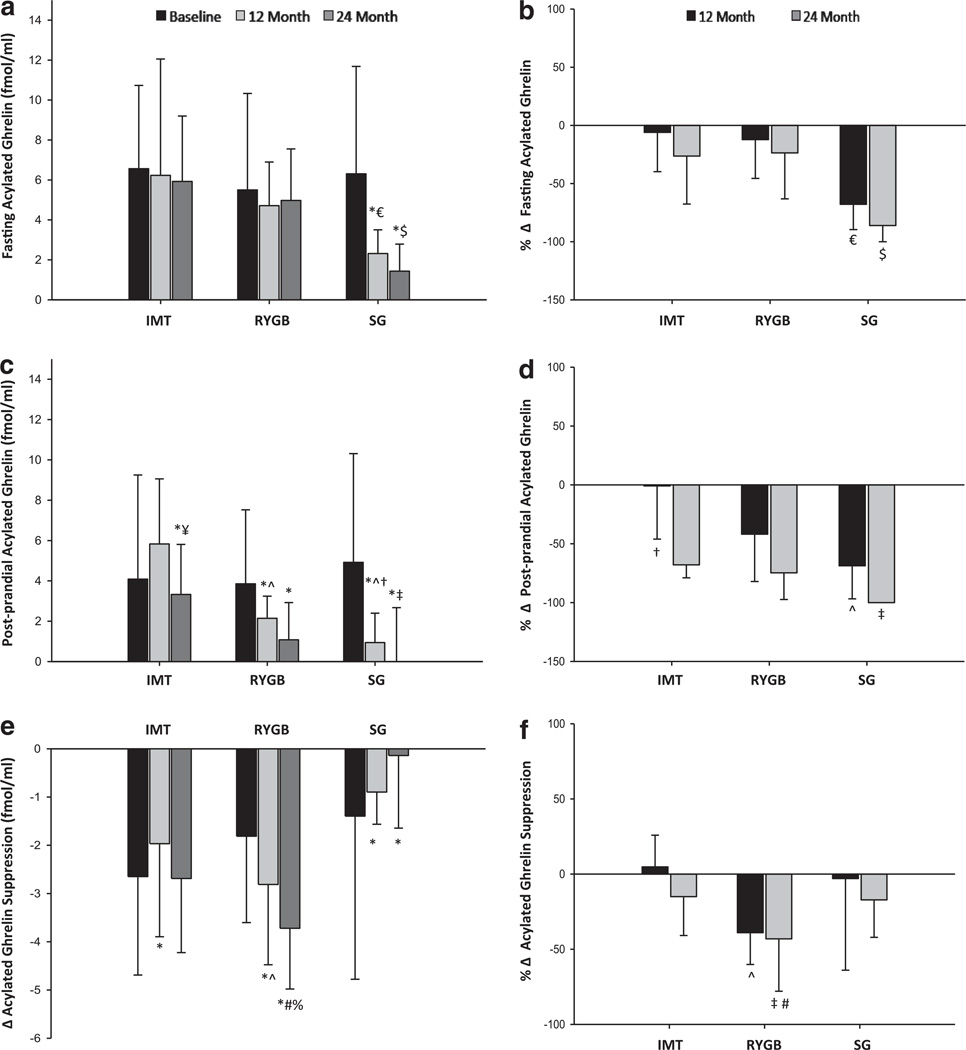
Results: RYGB and SG reduced body fat comparably (15-23 kg) at 12 and 24 months, whereas IMT had no effect. Beta-cell function increased 5.8-fold in RYGB and was greater than IMT at 24 months (P<0.001). However, there was no difference in insulin secretion between SG vs IMT at 24 months (P=0.32). Fasting AG was reduced fourfold following SG (P<0.01) and did not change with RYGB or IMT at 24 months. AG suppression improved more following RYGB than SG or IMT at 24 months (P=0.01 vs SG, P=0.07 vs IMT). At 24 months, AG suppression was associated with increased postprandial glucagon-like peptide-1 (r=-0.32, P<0.02) and decreased android fat (r=0.38; P<0.006).
Conclusions: Enhanced AG suppression persists for up to 2 years after RYGB, and this effect is associated with decreased android obesity and improved insulin secretion. Together, these findings suggest that AG suppression is partly responsible for the improved glucose control after RYGB surgery.
Conflict of interest statement
All the other authors declare no conflict of interest.
Figures


References
-
- Kahn SE, Hull RL, Utzschneider KM. Mechanisms linking obesity to insulin resistance and type 2 diabetes. Nature. 2006;444:840–846. - PubMed
-
- Buchwald H, Oien DM. Metabolic/bariatric surgery Worldwide 2008. Obesity Surg. 2009;19:1605–1611. - PubMed
-
- Mingrone G, Panunzi S, De Gaetano A, Guidone C, Iaconelli A, Leccesi L, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012;366:1577–1585. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
