

Costs and outcomes evaluation of patient navigation after abnormal cancer screening: evidence from the Patient Navigation Research Program
- PMID: 24166217
- PMCID: PMC3946403
- DOI: 10.1002/cncr.28438
Costs and outcomes evaluation of patient navigation after abnormal cancer screening: evidence from the Patient Navigation Research Program
Abstract
Background: Navigators can facilitate timely access to cancer services, but to the authors' knowledge there are little data available regarding their economic impact.
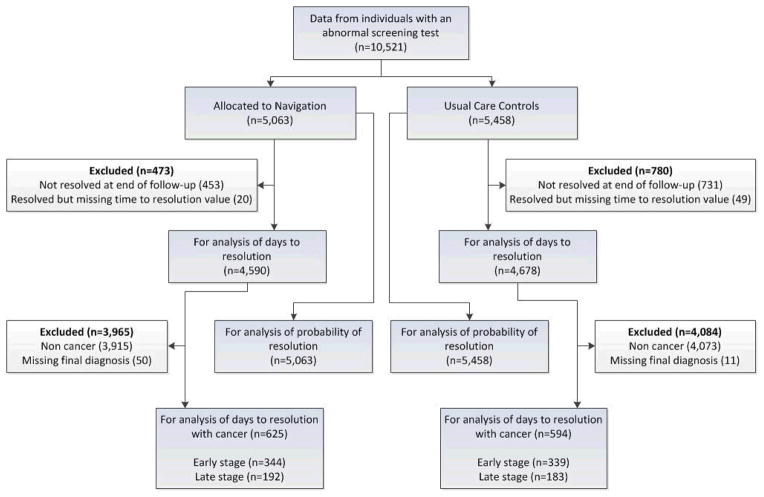
Methods: The authors conducted a cost-consequence analysis of navigation versus usual care among 10,521 individuals with abnormal breast, cervical, colorectal, or prostate cancer screening results who enrolled in the Patient Navigation Research Program study from January 1, 2006 to March 31, 2010. Navigation costs included diagnostic evaluation, patient and staff time, materials, and overhead. Consequences or outcomes were time to diagnostic resolution and probability of resolution. Differences in costs and outcomes were evaluated using multilevel, mixed-effects regression modeling adjusting for age, race/ethnicity, language, marital status, insurance status, cancer, and site clustering.
Results: The majority of individuals were members of a minority (70.7%) and uninsured or publically insured (72.7%). Diagnostic resolution was higher for navigation versus usual care at 180 days (56.2% vs 53.8%; P = .008) and 270 days (70.0% vs 68.2%; P < .001). Although there were no differences in the average number of days to resolution between the 2 groups (110 days vs 109 days; P = .63), the probability of ever having diagnostic resolution was higher for the navigation group versus the usual-care group (84.5% vs 79.6%; P < .001). The added cost of navigation versus usual care was $275 per patient (95% confidence interval, $260-$290; P < .001). There was no significant difference in stage distribution among the 12.4% of patients in the navigation group vs 11% of the usual-care patients diagnosed with cancer.
Conclusions: Navigation adds costs and modestly increases the probability of diagnostic resolution among patients with abnormal screening test results. Navigation is only likely to be cost-effective if improved resolution translates into an earlier cancer stage at the time of diagnosis.
Keywords: abnormal cancer screening; cancer; cost; navigation; outcomes.
© 2013 American Cancer Society.
Conflict of interest statement
Conflicts of Interest: None declared
Figures
References
-
- Shavers VL, Fagan P, McDonald P. Health disparities across the cancer continuum. J Health Care Poor Underserved. 2007 Nov;18(4 Suppl):1–5. - PubMed
-
- Yabroff KR, Washington KS, Leader A, Neilson E, Mandelblatt J. Is the promise of cancer-screening programs being compromised? Quality of follow-up care after abnormal screening results. Med Care Res Rev. 2003 Sep;60(3):294–331. - PubMed
-
- Baig N, Myers RE, Turner BJ, et al. Physician-reported reasons for limited follow-up of patients with a positive fecal occult blood test screening result. American Journal of Gastroenterology. 2003 Sep;98(9):2078–2081. - PubMed
-
- Morris JB, Stellato TA, Guy BB, Gordon NH, Berger NA. A critical analysis of the largest reported mass fecal occult blood screening program in the United States. American Journal of Surgery. 1991 Jan;161(1):101–105. discussion 105–106. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 CA152958/CA/NCI NIH HHS/United States
- U01 CA116875/CA/NCI NIH HHS/United States
- U01CA116925/CA/NCI NIH HHS/United States
- U01 CA114593/CA/NCI NIH HHS/United States
- U01CA116903/CA/NCI NIH HHS/United States
- U01 CA116924/CA/NCI NIH HHS/United States
- U01CA116924/CA/NCI NIH HHS/United States
- U01 CA116937/CA/NCI NIH HHS/United States
- U01 CA116925/CA/NCI NIH HHS/United States
- U01 CA117281/CA/NCI NIH HHS/United States
- U01CA116937/CA/NCI NIH HHS/United States
- U01 CA116885/CA/NCI NIH HHS/United States
- U01 CA116903/CA/NCI NIH HHS/United States
- U01 CA088283/CA/NCI NIH HHS/United States
- KL2 TR001118/TR/NCATS NIH HHS/United States
- U01 CA116892/CA/NCI NIH HHS/United States
- P30 CA016058/CA/NCI NIH HHS/United States
- K01 CA134554/CA/NCI NIH HHS/United States
- K05 CA096940/CA/NCI NIH HHS/United States
- UL1 TR001120/TR/NCATS NIH HHS/United States
- U01CA116885/CA/NCI NIH HHS/United States
- U01CA116875/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
