

Practice patterns and long-term survival for early-stage rectal cancer
- PMID: 24166526
- PMCID: PMC3837090
- DOI: 10.1200/JCO.2013.49.1860
Practice patterns and long-term survival for early-stage rectal cancer
Abstract
Purpose: Standard of care treatment for most stage I rectal cancers is total mesorectal excision (TME). Given the morbidity associated with TME, local excision (LE) for early-stage rectal cancer has been explored. This study examines practice patterns and overall survival (OS) for early-stage rectal cancer.
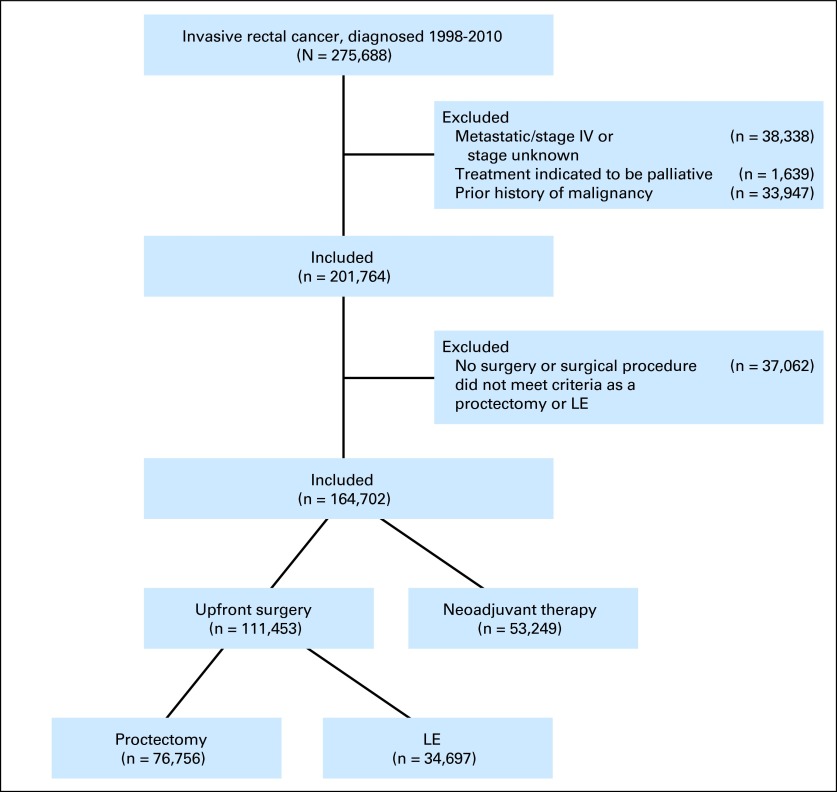
Methods: All patients in the National Cancer Data Base diagnosed with rectal cancer from 1998 to 2010 were initially included. Use of LE versus proctectomy and use of adjuvant radiation therapy were compared over time. Adjusted Cox proportional hazards models were used to compare OS based on treatment.
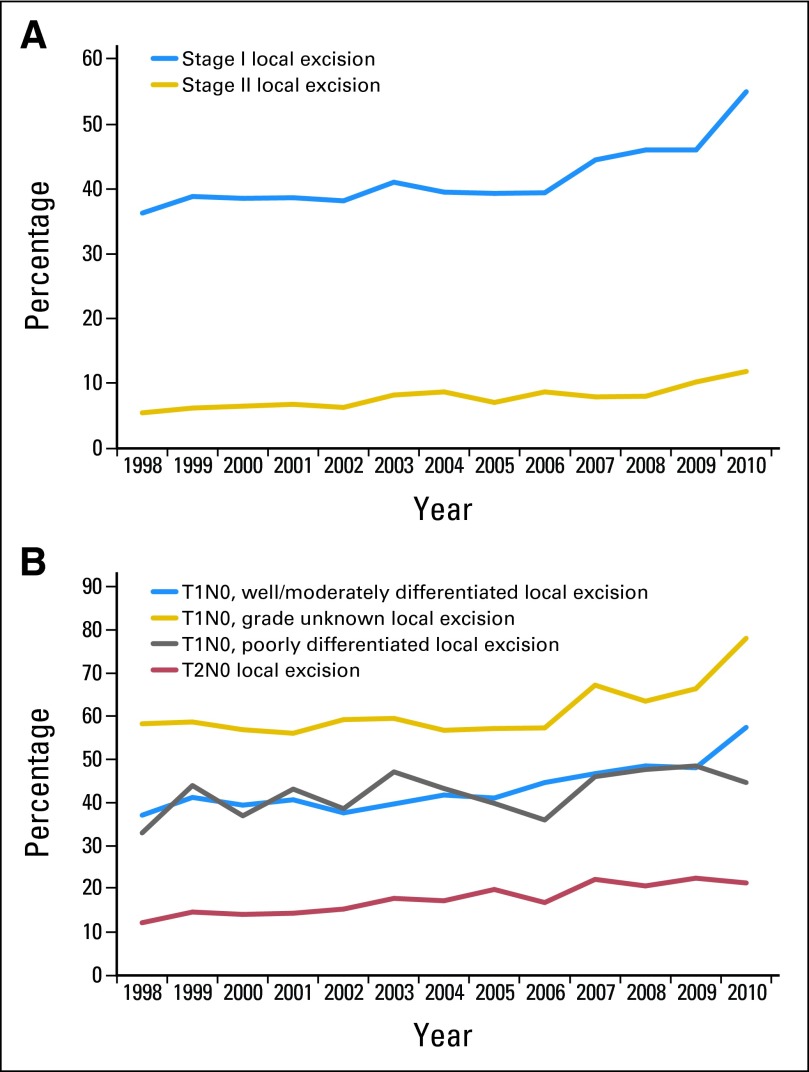
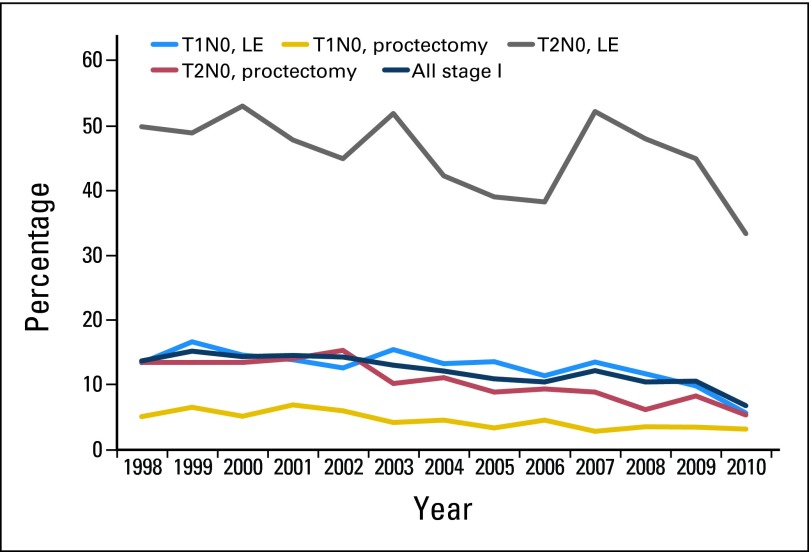
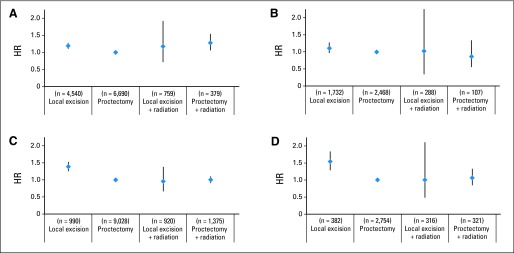
Results: LE was used to treat 46.5% of patients with T1 and 16.8% with T2 tumors. Use of LE increased steadily over time (P < .001). LE was most commonly used for women, black patients, very old patients, those without private health insurance, those with well-differentiated tumors, and those with T1 tumors. Proctectomy was associated with higher rates of tumor-free surgical margins compared with LE (95% v 76%; P < .001). Adjuvant radiation therapy use decreased over time independent of surgical procedure or T stage. For T2N0 disease, patients treated with LE alone had significantly poorer adjusted OS than those treated with proctectomy alone or multimodality therapy.
Conclusion: Guideline-concordant adoption of LE for treatment of low-risk stage I rectal cancer is increasing. However, use of LE is also increasing for higher-risk rectal cancers that do not meet guideline criteria for LE. Treatment with LE alone is associated with poorer long-term OS. Additional studies are warranted to understand the factors driving increased use of LE.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Total mesorectal neglect in the age of total mesorectal excision.J Clin Oncol. 2013 Dec 1;31(34):4273-5. doi: 10.1200/JCO.2013.52.6434. Epub 2013 Oct 28. J Clin Oncol. 2013. PMID: 24166519 No abstract available.
References
-
- MacFarlane JK, Ryall RD, Heald RJ. Mesorectal excision for rectal cancer. Lancet. 1993;341:457–460. - PubMed
-
- Bleier JI, Maykel JA. Outcomes following proctectomy. Surg Clin North Am. 2013;93:89–106. - PubMed
-
- You YN. Local excision: Is it an adequate substitute for radical resection in T1/T2 patients? Semin Radiat Oncol. 2011;21:178–184. - PubMed
-
- Nash GM, Weiser MR, Guillem JG, et al. Long-term survival after transanal excision of T1 rectal cancer. Dis Colon Rectum. 2009;52:577–582. - PubMed
-
- Saraste D, Gunnarsson U, Janson M. Predicting lymph node metastases in early rectal cancer. Eur J Cancer. 2013;49:1104–1108. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
