Evaluation of electronic health record implementation in ophthalmology at an academic medical center (an American Ophthalmological Society thesis)
- PMID: 24167326
- PMCID: PMC3797873
Evaluation of electronic health record implementation in ophthalmology at an academic medical center (an American Ophthalmological Society thesis)
Abstract
Purpose: To evaluate three measures related to electronic health record (EHR) implementation: clinical volume, time requirements, and nature of clinical documentation. Comparison is made to baseline paper documentation.
Methods: An academic ophthalmology department implemented an EHR in 2006. A study population was defined of faculty providers who worked the 5 months before and after implementation. Clinical volumes, as well as time length for each patient encounter, were collected from the EHR reporting system. To directly compare time requirements, two faculty providers who utilized both paper and EHR systems completed time-motion logs to record the number of patients, clinic time, and nonclinic time to complete documentation. Faculty providers and databases were queried to identify patient records containing both paper and EHR notes, from which three cases were identified to illustrate representative documentation differences.
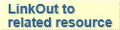
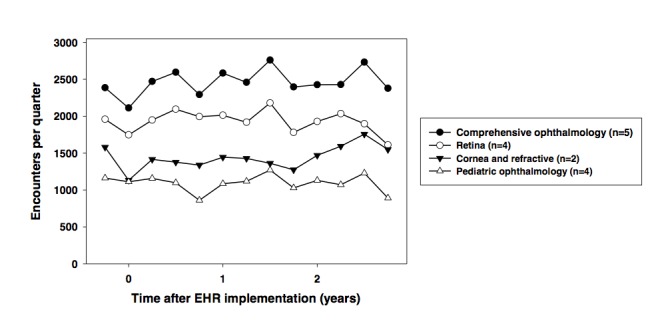
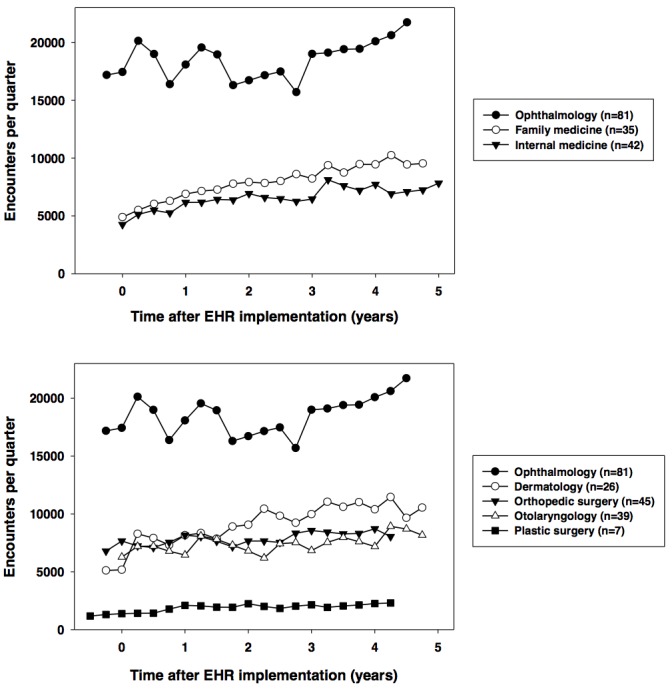
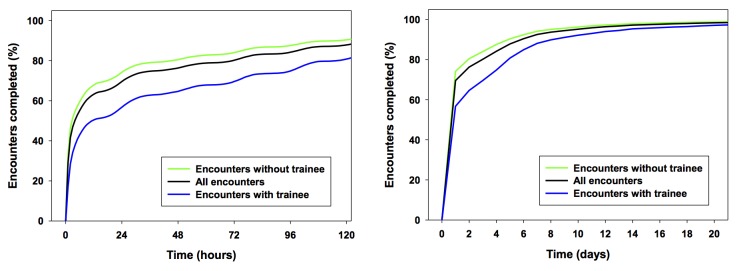
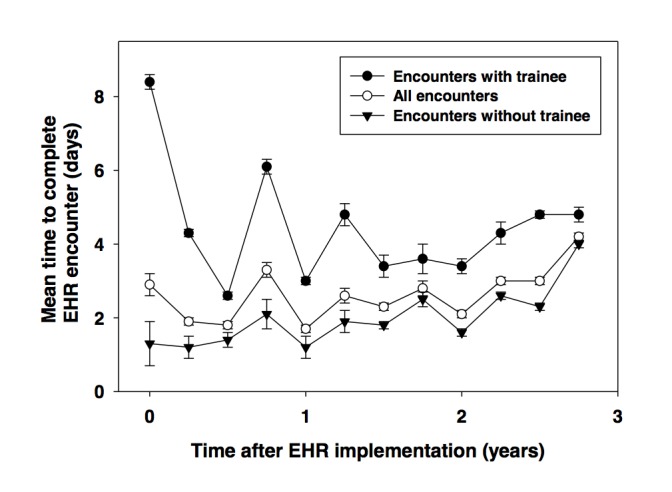
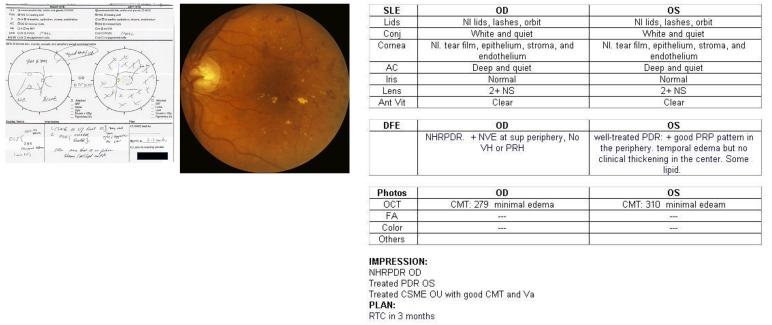
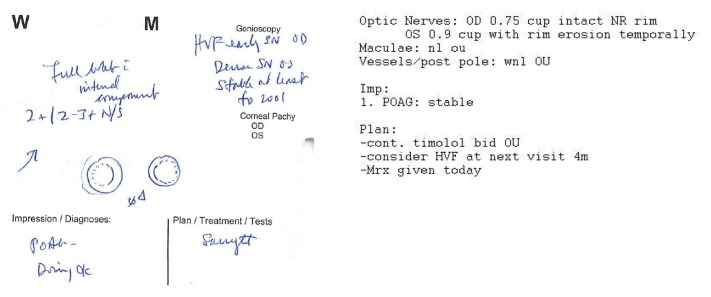
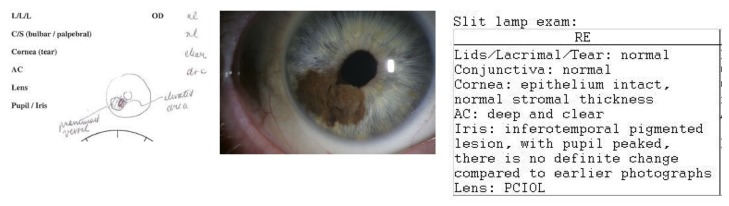
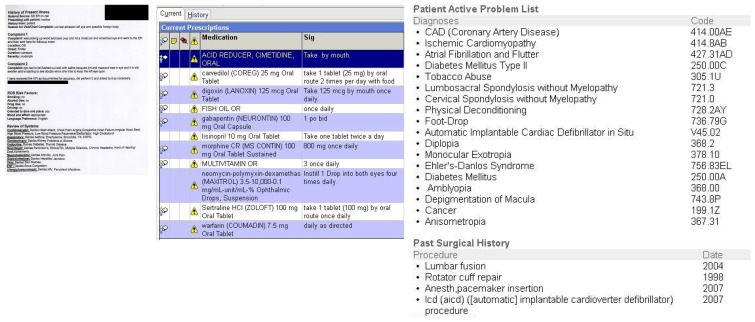
Results: Twenty-three faculty providers completed 120,490 clinical encounters during a 3-year study period. Compared to baseline clinical volume from 3 months pre-implementation, the post-implementation volume was 88% in quarter 1, 93% in year 1, 97% in year 2, and 97% in year 3. Among all encounters, 75% were completed within 1.7 days after beginning documentation. The mean total time per patient was 6.8 minutes longer with EHR than paper (P<.01). EHR documentation involved greater reliance on textual interpretation of clinical findings, whereas paper notes used more graphical representations, and EHR notes were longer and included automatically generated text.
Conclusion: This EHR implementation was associated with increased documentation time, little or no increase in clinical volume, and changes in the nature of ophthalmic documentation.
Figures
References
-
- Greenes RA, Shortliffe EH. Medical informatics: an emerging academic discipline and institutional priority. JAMA. 1990;263(8):1114–1120. - PubMed
-
- Committee on Quality of Health Care in America, Institute of Medicine . To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000. p. 1.
-
- Kassirer JP. The next transformation in the delivery of health care. N Engl J Med. 1995;332(1):52–54. - PubMed
-
- Institute for Health and Aging, University of California, San Francisco . Chronic Care in America: A 21st Century Challenge. Princeton, NJ: Robert Wood Johnson Foundation; 1996. p. 13. Available at: www.rwjf.org/files/publications/other/ChronicCareinAmerica.pdf. Accessed May 6, 2011.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources