

Elimination of HIV in South Africa through expanded access to antiretroviral therapy: a model comparison study
- PMID: 24167449
- PMCID: PMC3805487
- DOI: 10.1371/journal.pmed.1001534
Elimination of HIV in South Africa through expanded access to antiretroviral therapy: a model comparison study
Abstract
Background: Expanded access to antiretroviral therapy (ART) using universal test and treat (UTT) has been suggested as a strategy to eliminate HIV in South Africa within 7 y based on an influential mathematical modeling study. However, the underlying deterministic model was criticized widely, and other modeling studies did not always confirm the study's finding. The objective of our study is to better understand the implications of different model structures and assumptions, so as to arrive at the best possible predictions of the long-term impact of UTT and the possibility of elimination of HIV.
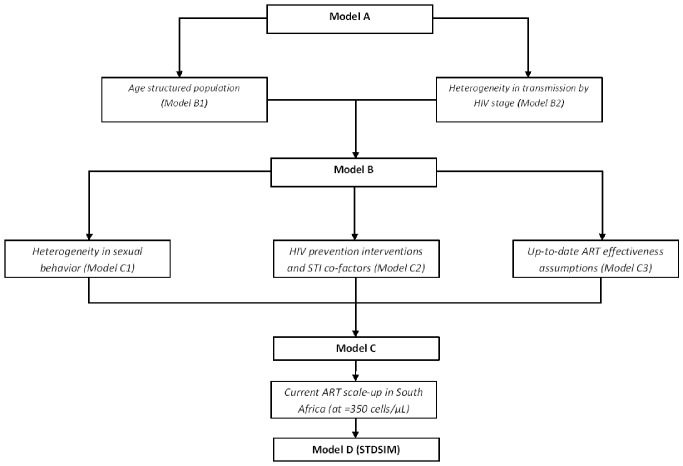
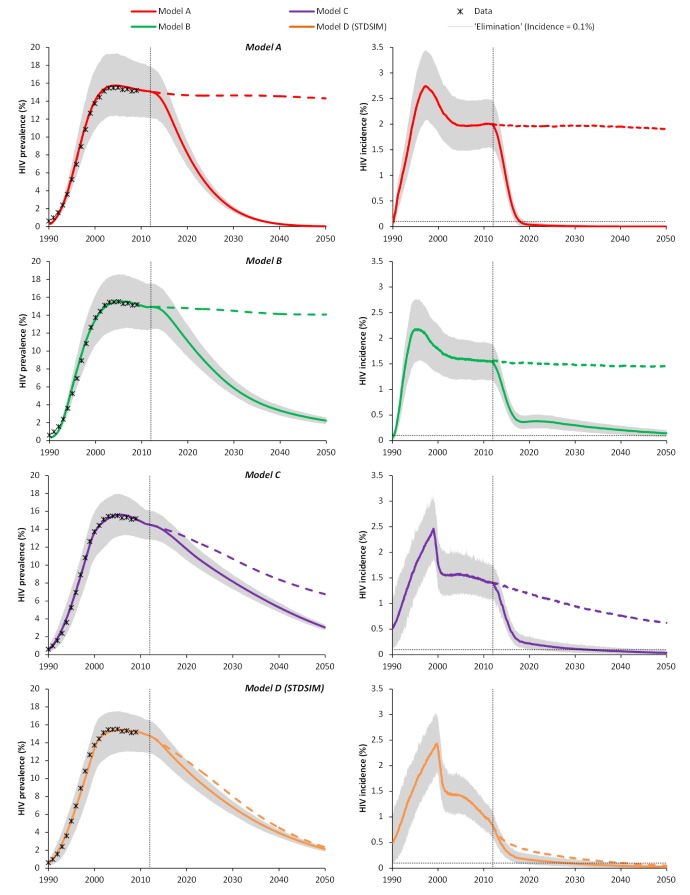
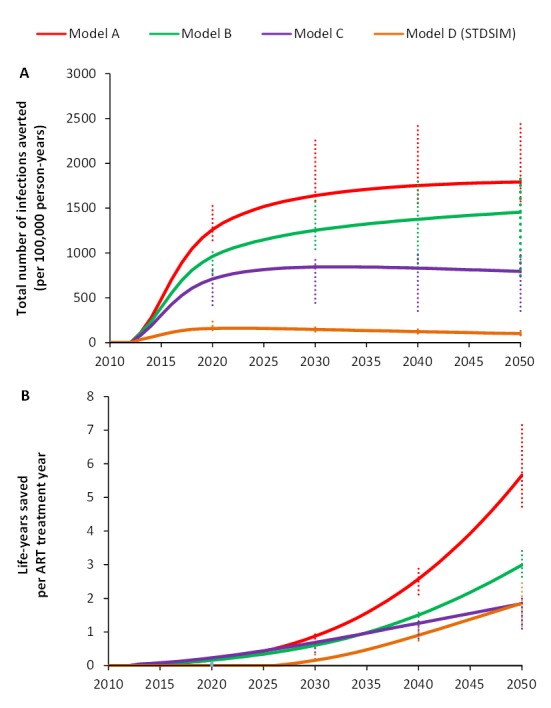
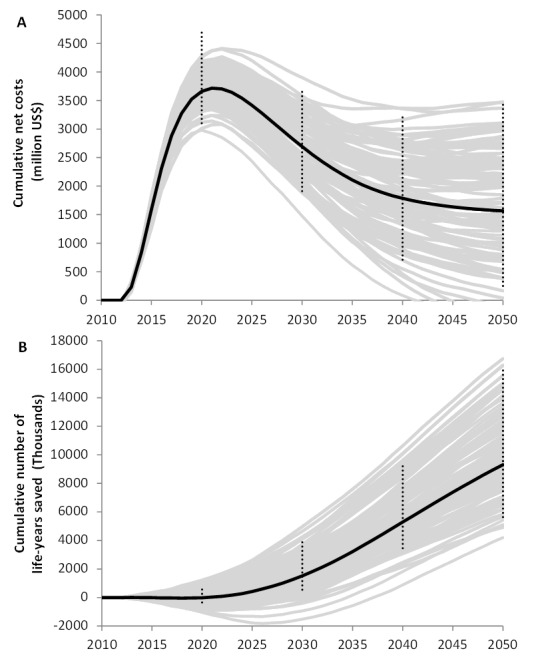
Methods and findings: We developed nine structurally different mathematical models of the South African HIV epidemic in a stepwise approach of increasing complexity and realism. The simplest model resembles the initial deterministic model, while the most comprehensive model is the stochastic microsimulation model STDSIM, which includes sexual networks and HIV stages with different degrees of infectiousness. We defined UTT as annual screening and immediate ART for all HIV-infected adults, starting at 13% in January 2012 and scaled up to 90% coverage by January 2019. All models predict elimination, yet those that capture more processes underlying the HIV transmission dynamics predict elimination at a later point in time, after 20 to 25 y. Importantly, the most comprehensive model predicts that the current strategy of ART at CD4 count ≤350 cells/µl will also lead to elimination, albeit 10 y later compared to UTT. Still, UTT remains cost-effective, as many additional life-years would be saved. The study's major limitations are that elimination was defined as incidence below 1/1,000 person-years rather than 0% prevalence, and drug resistance was not modeled.
Conclusions: Our results confirm previous predictions that the HIV epidemic in South Africa can be eliminated through universal testing and immediate treatment at 90% coverage. However, more realistic models show that elimination is likely to occur at a much later point in time than the initial model suggested. Also, UTT is a cost-effective intervention, but less cost-effective than previously predicted because the current South African ART treatment policy alone could already drive HIV into elimination. Please see later in the article for the Editors' Summary.
Conflict of interest statement
TBH and MLN are members of the
Figures
Comment in
-
Modelling the strategic use of antiretroviral therapy for the treatment and prevention of HIV.PLoS Med. 2013 Oct;10(10):e1001535. doi: 10.1371/journal.pmed.1001535. Epub 2013 Oct 22. PLoS Med. 2013. PMID: 24167450 Free PMC article.
References
-
- Joint United Nations Programme on HIV/AIDS (2012) Report on the global AIDS epidemic 2012. Geneva: Joint United Nations Programme on HIV/AIDS.
-
- Rehle TM, Hallett TB, Shisana O, Pillay-van Wyk V, Zuma K, et al. (2010) A decline in new HIV infections in South Africa: estimating HIV incidence from three national HIV surveys in 2002, 2005 and 2008. PLoS ONE 5: e11094 doi:10.1371/journal.pone.0011094 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
